Saha Sandeep A, Krishnan Kousik, Madias Christopher, Trohman Richard G
Section of Cardiac Electrophysiology, Division of Cardiology, Department of Medicine, Rush University Medical Center, Chicago, IL, USA.
Cardiol Ther. 2016 Dec;5(2):229-243. doi: 10.1007/s40119-016-0072-4. Epub 2016 Sep 19.
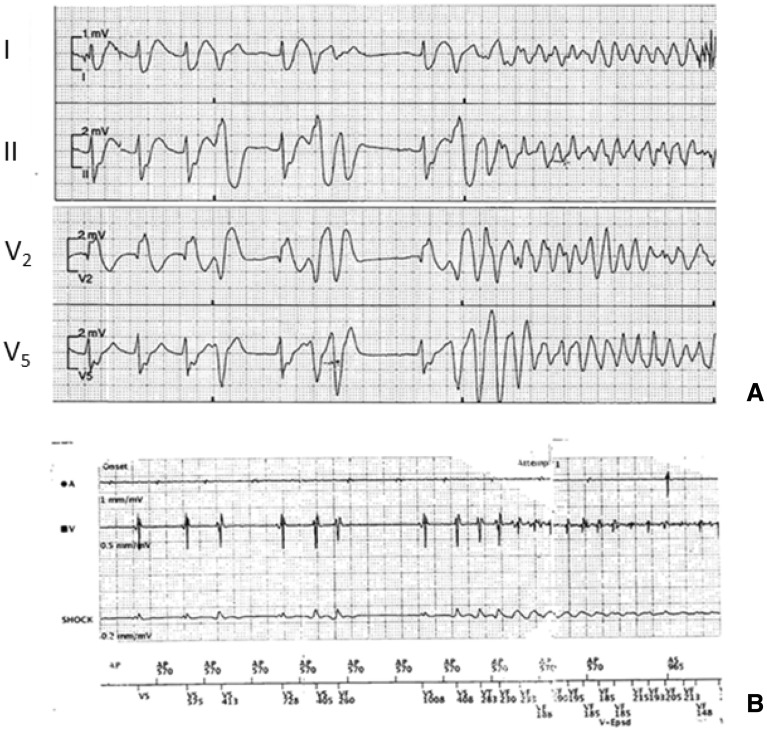
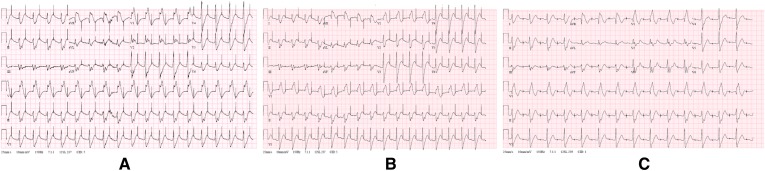
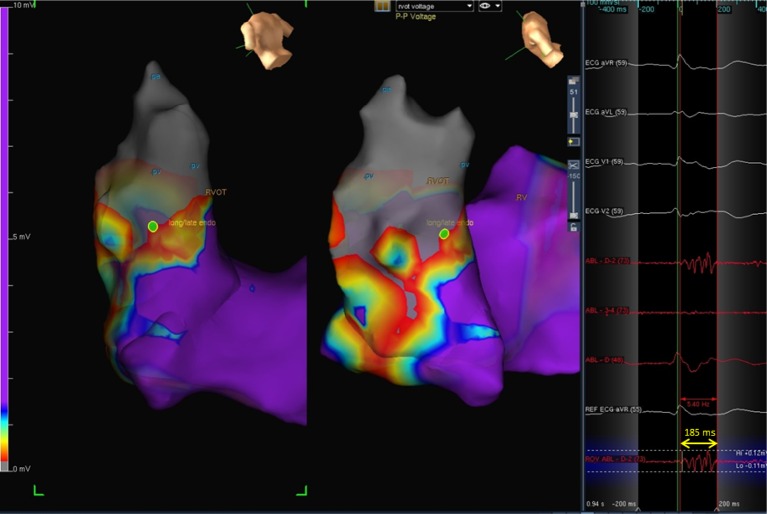
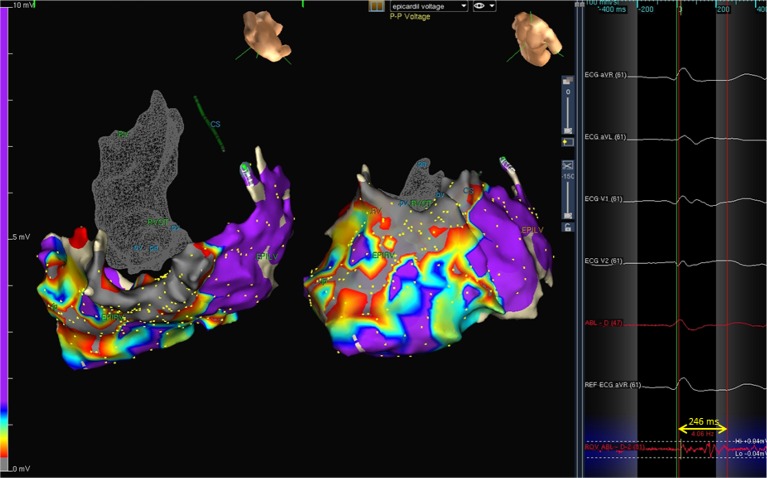
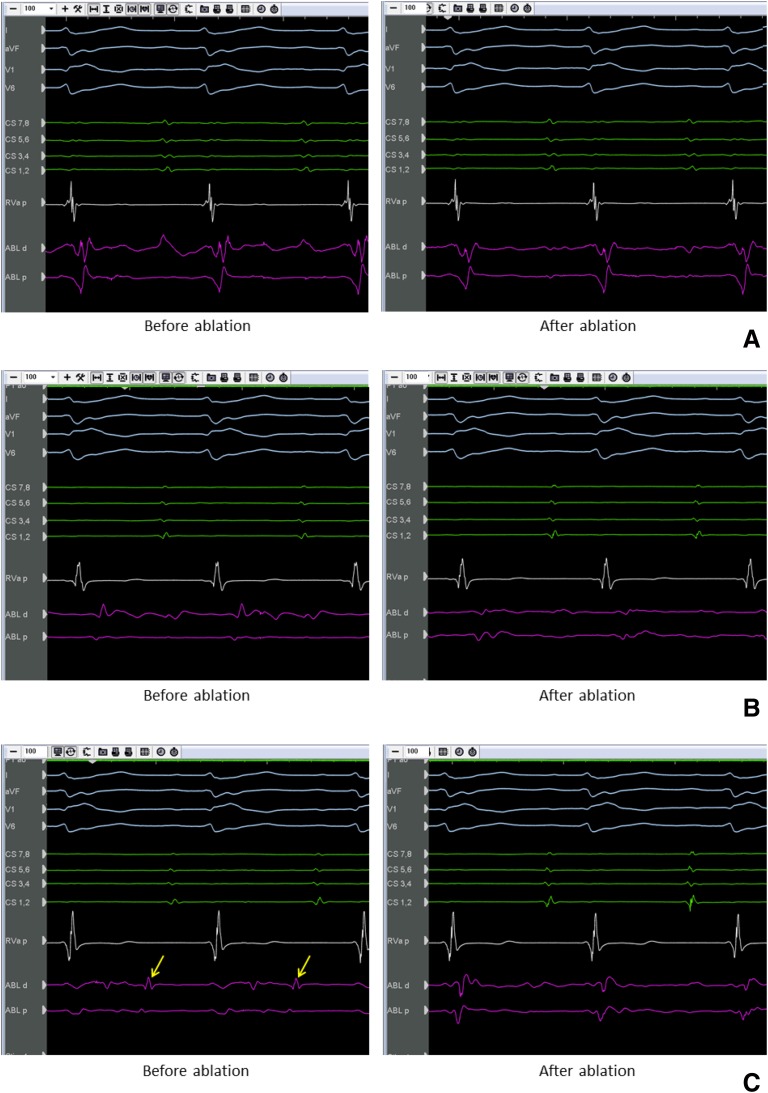
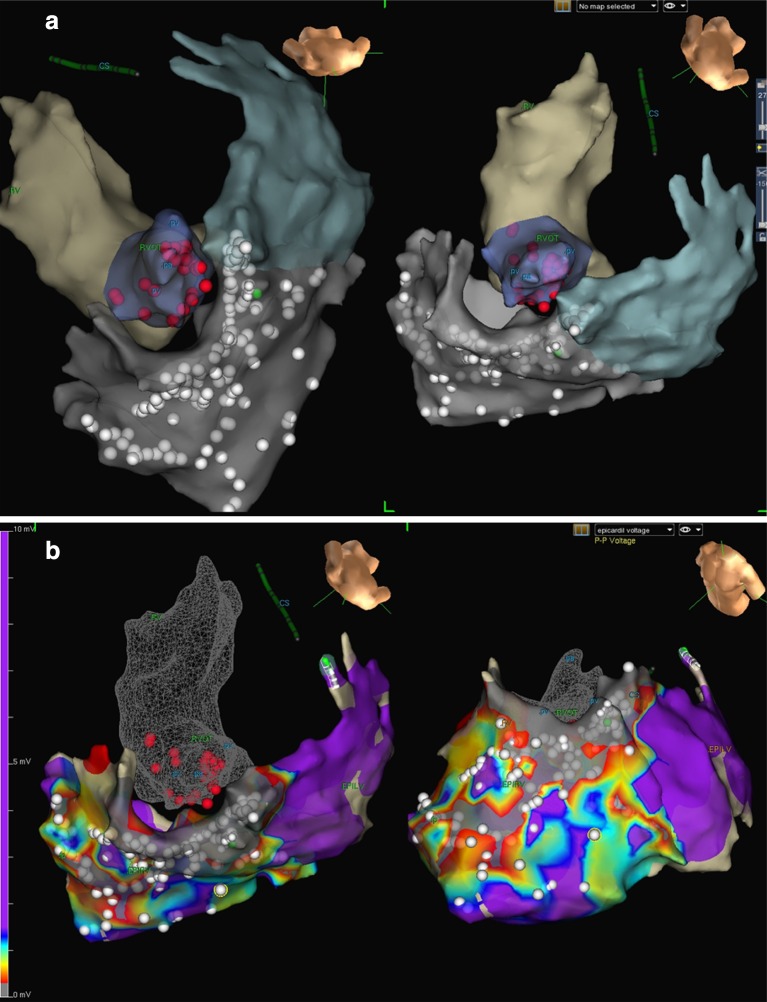
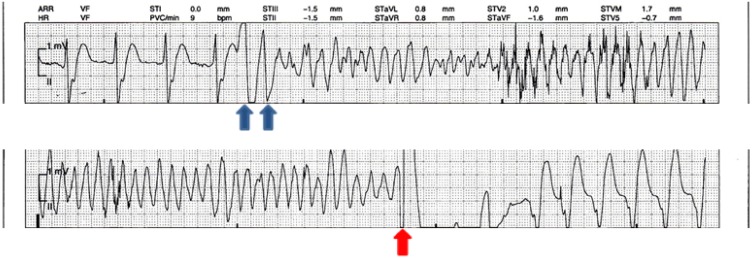
A 34-year-old man with Brugada syndrome (BrS) presented with electrical storm, manifested as multiple appropriate shocks from his implantable cardioverter-defibrillator over a period of 7 hours. He had not tolerated prior treatment with quinidine, and had self-discontinued cilostazol citing persistent palpitations. After stabilization with intravenous isoproterenol, an electrophysiology study was performed but no spontaneous or induced ventricular ectopic beats were identified. A three-dimensional (3D) endocardial electro-anatomic map of the right ventricular outflow tract (RVOT), pulmonic valve, and pulmonary artery, as well as a 3D epicardial map of the RVOT, were created. Low voltage, complex, fractionated electrograms and late potentials were targeted for irrigated radiofrequency ablation both endocardially and epicardially. Post-procedure, he was maintained on cilostazol (referring clinician preference), and has had no further ventricular tachyarrhythmia episodes over the past forty-one months. We propose that this novel ablation strategy may be useful for acute management of selected patients with BrS.
一名34岁的布加综合征(BrS)男性患者出现电风暴,表现为在7小时内其植入式心脏复律除颤器多次进行恰当电击。他之前不能耐受奎尼丁治疗,且因持续心悸自行停用了西洛他唑。在静脉注射异丙肾上腺素稳定病情后,进行了电生理研究,但未发现自发或诱发的室性异位搏动。创建了右心室流出道(RVOT)、肺动脉瓣和肺动脉的三维(3D)心内膜电解剖图,以及RVOT的3D心外膜图。低电压、复杂、碎裂电图和晚电位成为心内膜和心外膜灌注射频消融的靶点。术后,他继续服用西洛他唑(参考主治医生的偏好),在过去41个月里没有再次发生室性快速性心律失常事件。我们认为这种新型消融策略可能对部分BrS患者的急性治疗有用。