Das Sushmita, Alcock Glyn, Azad Kishwar, Kuddus Abdul, Manandhar Dharma S, Shrestha Bhim Prasad, Nair Nirmala, Rath Shibanand, More Neena Shah, Saville Naomi, Houweling Tanja A J, Osrin David
SNEHA (Society for Nutrition, Education and Health Action), 310, Urban Health Centre, 60 Feet Road, Dharavi, Mumbai, 400 017, Maharashtra, India.
UCL Institute for Global Health, 30 Guilford Street, London, WC1N 1EH, UK.
BMC Pregnancy Childbirth. 2016 Sep 20;16:273. doi: 10.1186/s12884-016-1069-7.
Maternity care in South Asia is available in both public and private sectors. Using data from demographic surveillance sites in Bangladesh, Nepal and rural and urban India, we aimed to compare institutional delivery rates and public-private share.
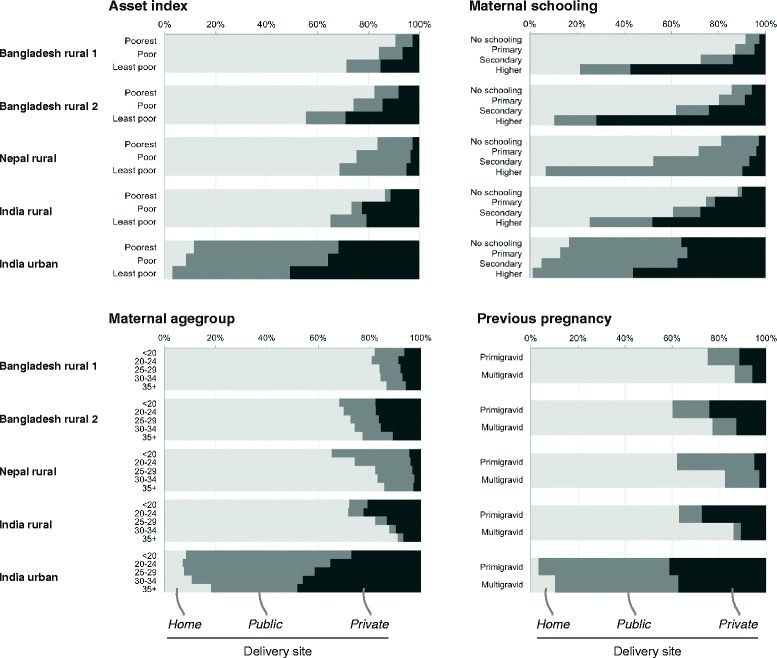
We used records of maternity care collected in socio-economically disadvantaged communities between 2005 and 2011. Institutional delivery was summarized by four potential determinants: household asset index, maternal schooling, maternal age, and parity. We developed logistic regression models for private sector institutional delivery with these as independent covariates.
The data described 52 750 deliveries. Institutional delivery proportion varied and there were differences in public-private split. In Bangladesh and urban India, the proportion of deliveries in the private sector increased with wealth, maternal education, and age. The opposite was observed in rural India and Nepal.
The proportion of institutional delivery increased with economic status and education. The choice of sector is more complex and provision and perceived quality of public sector services is likely to play a role. Choices for safe maternity are influenced by accessibility, quantity and perceived quality of care. Along with data linkage between private and public sectors, increased regulation should be part of the development of the pluralistic healthcare systems that characterize south Asia.
南亚的孕产妇保健服务由公共部门和私营部门共同提供。我们利用来自孟加拉国、尼泊尔以及印度农村和城市人口监测点的数据,旨在比较机构分娩率及公私部门所占比例。
我们使用了2005年至2011年期间在社会经济弱势社区收集的孕产妇保健记录。机构分娩由四个潜在决定因素进行总结:家庭资产指数、母亲受教育程度、母亲年龄和胎次。我们以这些因素作为独立协变量,建立了私营部门机构分娩的逻辑回归模型。
数据涵盖了52750例分娩。机构分娩比例各不相同,公私部门的划分也存在差异。在孟加拉国和印度城市,私营部门的分娩比例随财富、母亲教育程度和年龄的增加而上升。而在印度农村和尼泊尔则观察到相反的情况。
机构分娩比例随经济状况和教育程度的提高而增加。部门选择更为复杂,公共部门服务的提供和感知质量可能发挥了作用。安全孕产的选择受可及性、护理数量和感知质量的影响。除了公私部门之间的数据关联外,加强监管应成为南亚多元医疗体系发展的一部分。