Alcock Glyn, Das Sushmita, Shah More Neena, Hate Ketaki, More Sharda, Pantvaidya Shanti, Osrin David, Houweling Tanja A J
Institute for Global Health, University College London, 30 Guilford Street, London, WC1N 1EH, UK.
Society for Nutrition, Education and Health Action (SNEHA), 310, 3rd Floor, Urban Health Center, 60 Feet Road, Dharavi, Mumbai, 400 017, India.
BMC Pregnancy Childbirth. 2015 Sep 28;15:231. doi: 10.1186/s12884-015-0661-6.
Discussions of maternity care in developing countries tend to emphasise service uptake and overlook choice of provider. Understanding how families choose among health providers is essential to addressing inequitable access to care. Our objectives were to quantify the determinants and choice of maternity care provider in Mumbai's informal urban settlements, and to explore the reasons underlying their choices.
The study was conducted in informal urban communities in eastern Mumbai. We developed regression models using data from a census of married women aged 15-49 to test for associations between maternal characteristics and uptake of care and choice of provider. We then conducted seven focus group discussions and 16 in-depth interviews with purposively selected participants, and used grounded theory methods to examine the reasons for their choices.
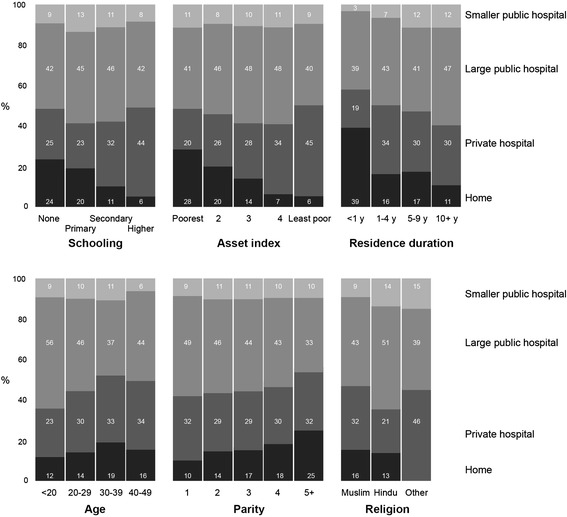
Three thousand eight hundred forty-eight women who had given birth in the preceding 2 years were interviewed in the census. The odds of institutional prenatal and delivery care increased with education, economic status, and duration of residence in Mumbai, and decreased with parity. Tertiary public hospitals were the commonest site of care, but there was a preference for private hospitals with increasing socio-economic status. Women were more likely to use tertiary public hospitals for delivery if they had fewer children and were Hindu. The odds of delivery in the private sector increased with maternal education, wealth, age, recent arrival in Mumbai, and Muslim faith. Four processes were identified in choosing a health care provider: exploring the options, defining a sphere of access, negotiating autonomy, and protective reasoning. Women seeking a positive health experience and outcome adopted strategies to select the best or most suitable, accessible provider.
In Mumbai's informal settlements, institutional maternity care is the norm, except among recent migrants. Poor perceptions of primary public health facilities often cause residents to bypass them in favour of tertiary hospitals or private sector facilities. Families follow a complex selection process, mediated by their ability to mobilise economic and social resources, and a concern for positive experiences of health care and outcomes. Health managers must ensure quality services, a functioning regulatory mechanism, and monitoring of provider behaviour.
关于发展中国家孕产妇保健的讨论往往侧重于服务利用情况,而忽视了提供者的选择。了解家庭如何在医疗服务提供者之间进行选择对于解决医疗服务获取不平等问题至关重要。我们的目标是量化孟买城市非正式住区孕产妇保健提供者的决定因素和选择情况,并探究其选择背后的原因。
该研究在孟买东部的城市非正式社区开展。我们利用15至49岁已婚女性普查数据建立回归模型,以检验孕产妇特征与保健利用及提供者选择之间的关联。然后,我们对有目的地挑选出的参与者进行了七次焦点小组讨论和16次深入访谈,并采用扎根理论方法研究其选择原因。
在普查中,对之前两年内分娩的3848名女性进行了访谈。机构产前和分娩保健的几率随着教育程度、经济状况以及在孟买的居住时长而增加,随着胎次而降低。三级公立医院是最常见的保健场所,但随着社会经济地位的提高,对私立医院的偏好增加。如果孩子较少且是印度教徒,女性更有可能在三级公立医院分娩。在私立部门分娩的几率随着孕产妇教育程度、财富、年龄、刚到孟买以及穆斯林信仰而增加。在选择医疗服务提供者时确定了四个过程:探索选择、界定获取范围、协商自主权和保护性推理。寻求积极健康体验和结果的女性采取策略选择最佳或最合适、可及的提供者。
在孟买的非正式住区,除了新移民外,机构孕产妇保健是常态。对初级公共卫生设施的不良认知常常导致居民绕过这些设施,转而选择三级医院或私立部门设施。家庭遵循一个复杂的选择过程,这一过程由他们调动经济和社会资源的能力以及对积极医疗保健体验和结果的关注所介导。卫生管理人员必须确保优质服务、有效的监管机制以及对提供者行为的监督。