Gender and Women's Health Unit, Centre for Health Equity, School of Population and Global Health, The University of Melbourne, Melbourne, Victoria, Australia
Disability and Health Unit, Centre for Health Equity, School of Population and Global Health, The University of Melbourne, Melbourne, Victoria, Australia.
BMJ Glob Health. 2020 Dec;5(12). doi: 10.1136/bmjgh-2020-003844.
Caesarean section (CS) rates are increasing globally. CS can be a live-saving procedure when medically indicated, but it comes with higher risks for women and newborns when done without medical indication. Crucially, inequalities in who receives CS exist, both within and across countries. Understanding factors driving increasing rates and inequalities of CS is imperative to optimise the use of this life-saving intervention. This study aimed to investigate trends of CS use and inequalities across sociodemographic characteristics in Indonesia over a 30-year period.
Seven waves of the Indonesia Demographic and Health Survey were used to estimate trends and inequalities in CS from 1987 to 2017. Relative and absolute inequalities across a range of sociodemographic characteristics were estimated and trends in inequalities were assessed through changes in rate ratio and rate difference.
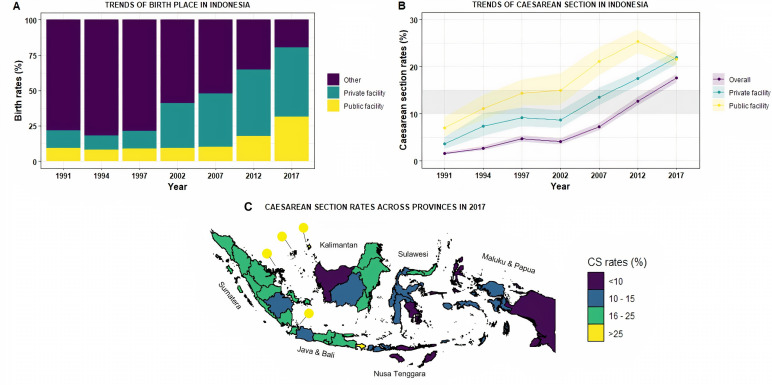
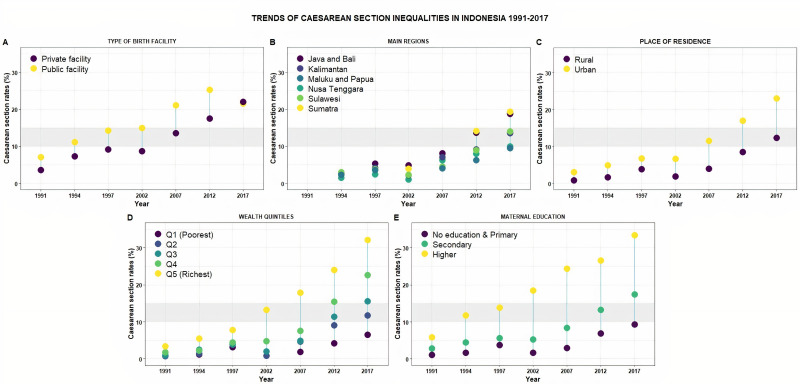
The proportion of facility-based births in Indonesia has increased in the past 30 years, coinciding with an increase in CS rate (CSR) (1991 CSR: 1.6% (95% CI 1.3 to 1.9); 2017 CSR: 17.6% (95% CI 16.7 to 18.5)). Higher rates of CS are observed mostly in Western Indonesia, while lower CSRs are observed in Eastern Indonesia. Inequalities of CSRs in Indonesia are observed across type of health facility (public/private), regions, places of residence, wealth quintiles and maternal education, with the highest CSRs in more affluent and educated groups. Widening absolute inequalities of CS are observed across all sociodemographic characteristics, except facility type, where CSR gaps between public and private facilities have closed on both relative and absolute scales.
This study provides evidence of increasing trends in CSRs and widening absolute inequalities in CSRs across different sociodemographic groups of women in Indonesia. The context of increasing CSRs across society, however, may have resulted in more stable relative inequalities. Improving understanding of the drivers of these trends in Indonesia and, particularly, of women's and providers' perspectives and preferences for childbirth, should be prioritised to optimise the use of CS.
全球剖宫产率不断上升。当医学指征明确时,剖宫产可以是一种救命的手术,但如果没有医学指征而进行剖宫产,母婴风险会更高。至关重要的是,在国家内部和国家之间,谁接受剖宫产存在不平等现象。了解推动剖宫产率和不平等现象增加的因素对于优化这种救命干预措施的使用至关重要。本研究旨在调查 30 年来印度尼西亚剖宫产使用率和社会人口特征不平等的趋势。
本研究使用了 7 次印度尼西亚人口与健康调查的数据,以估计 1987 年至 2017 年期间剖宫产的使用趋势和社会人口特征不平等。通过比率差异和比率比值的变化来评估不平等的趋势,并对一系列社会人口特征的相对和绝对不平等进行估计。
在过去的 30 年里,印度尼西亚的医疗机构分娩比例有所增加,同时剖宫产率(CSR)也有所上升(1991 年 CSR:1.6%(95%CI 1.3 至 1.9);2017 年 CSR:17.6%(95%CI 16.7 至 18.5))。较高的剖宫产率主要出现在印度尼西亚西部,而较低的 CSR 则出现在东部。印度尼西亚的 CSR 不平等现象存在于医疗机构类型(公立/私立)、地区、居住地、财富五分位数和产妇教育程度等方面,最富裕和受教育程度较高的群体的 CSR 率最高。在所有社会人口特征中,剖宫产率的绝对不平等差距都在扩大,除了医疗机构类型,因为公立和私立医疗机构之间的 CSR 差距在相对和绝对两个尺度上都在缩小。
本研究提供了证据表明,印度尼西亚不同社会人口群体的 CSR 呈上升趋势,CSR 的绝对不平等也在扩大。然而,由于社会整体上的 CSR 增加,相对不平等可能更加稳定。优先了解这些趋势的驱动因素,特别是了解妇女和提供者对分娩的观点和偏好,应该是优化剖宫产使用的重点。