Singh Jasvinder A, Yu Shaohua
Medicine Service, Birmingham VA Medical Center, Birmingham, AL, USA.
Department of Medicine at School of Medicine, and Division of Epidemiology at School of Public Health, University of Alabama at Birmingham (UAB), Faculty Office Tower 805B, 510 20th Street S, Birmingham, AL, 35294, USA.
Arthritis Res Ther. 2016 Sep 22;18(1):209. doi: 10.1186/s13075-016-1111-1.
Previous observational studies that have examined the association of allopurinol with myocardial infarction (MI) have provided contradictory results. One study showed that allopurinol reduced the risk, while another study showed an increased risk with allopurinol. Therefore, our objective was to assess whether allopurinol use is associated with a reduction in the risk of MI in the elderly.
We used the 2006-2012 5 % random sample of Medicare beneficiaries to study the association of new allopurinol initiation and the risk of incident MI in a cohort study. Multivariable-adjusted Cox regression models adjusted for age, gender, race, and Charlson index, in addition to various cardio-protective medications (beta-blockers, angiotensin-converting enzyme (ACE) inhibitors, diuretics, statins). We calculated hazard ratios (HRs) with 95 % confidence intervals (CIs). Sensitivity analyses adjusted for coronary artery disease (CAD) risk factors, including hypertension, hyperlipidemia, diabetes, and smoking.
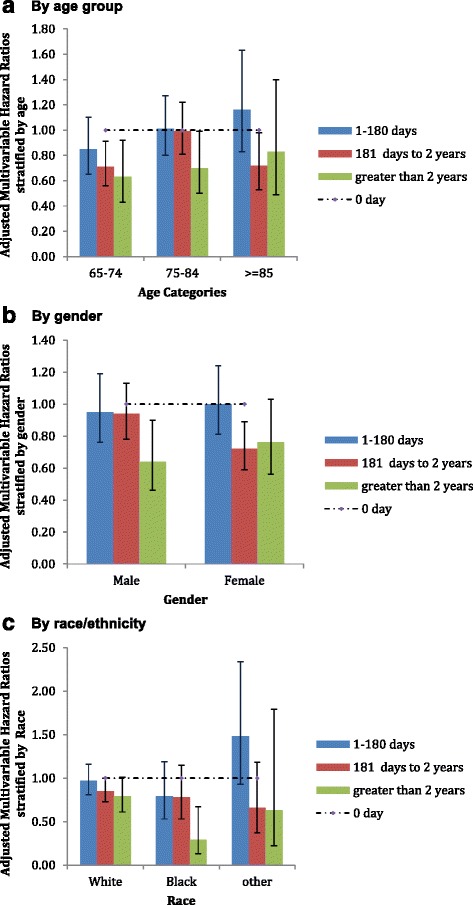
Of the 29,298 episodes of incident allopurinol use, 1544 were associated with incident MI (5.3 % episodes). Allopurinol use was associated with reduced hazards of MI, with a HR of 0.85 (95 % CI, 0.77 to 0.95). Compared to no allopurinol use, longer durations of allopurinol use were associated with a lower HR of MI: 1-180 days, 0.98 (95 % CI, 0.84 to 1.14); 181 days to 2 years, 0.83 (95 % CI, 0.72 to 0.95); and >2 years, 0.70 (95 % CI, 0.56 to 0.88). Other factors associated with a higher hazard of MI were: age 75 to <85 years and ≥85 years, male gender, higher Charlson index score, and the use of an ACE inhibitor. Adjustment for CAD risk factors confirmed these findings.
Incident allopurinol use was associated with a reduction in the risk of incident MI in the elderly. Longer durations of allopurinol use reduced the risk of incident MI incrementally. Future studies should assess the underlying mechanisms for MI prevention and assess the risk-benefit ratio for allopurinol use.
以往关于别嘌醇与心肌梗死(MI)关联的观察性研究结果相互矛盾。一项研究表明别嘌醇可降低风险,而另一项研究则显示使用别嘌醇会增加风险。因此,我们的目标是评估使用别嘌醇是否与降低老年人患心肌梗死的风险相关。
我们使用2006 - 2012年医疗保险受益人的5%随机样本,在一项队列研究中研究新开始使用别嘌醇与新发心肌梗死风险之间的关联。多变量调整的Cox回归模型除了对各种心脏保护药物(β受体阻滞剂、血管紧张素转换酶(ACE)抑制剂、利尿剂、他汀类药物)进行调整外,还对年龄、性别、种族和查尔森指数进行了调整。我们计算了风险比(HRs)及95%置信区间(CIs)。敏感性分析对冠状动脉疾病(CAD)风险因素进行了调整,包括高血压、高脂血症、糖尿病和吸烟。
在29298例新使用别嘌醇的病例中,1544例与新发心肌梗死相关(占5.3%)。使用别嘌醇与心肌梗死风险降低相关,HR为0.85(95%CI,0.77至0.95)。与未使用别嘌醇相比,别嘌醇使用时间越长,心肌梗死的HR越低:1 - 180天,0.98(95%CI,0.84至1.14);181天至2年,0.83(95%CI,0.72至0.95);超过2年,0.70(95%CI,0.56至0.88)。与心肌梗死风险较高相关的其他因素包括:年龄75至<85岁及≥85岁、男性、查尔森指数评分较高以及使用ACE抑制剂。对CAD风险因素的调整证实了这些发现。
新使用别嘌醇与老年人新发心肌梗死风险降低相关。别嘌醇使用时间越长,新发心肌梗死风险逐渐降低。未来的研究应评估预防心肌梗死的潜在机制,并评估使用别嘌醇的风险效益比。