Goto Tadahiro, Camargo Carlos A, Hasegawa Kohei
Department of Emergency Medicine, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
Int J Chron Obstruct Pulmon Dis. 2016 Sep 7;11:2149-2155. doi: 10.2147/COPD.S110879. eCollection 2016.
Recent studies propose T2-mediated inflammation in patients with asthma-chronic obstructive pulmonary disease (COPD) overlap syndrome (ACOS). However, little is known about whether fractional exhaled nitric oxide (FeNO) differs between patients with ACOS and those with COPD alone. To address this knowledge gap, a nationally representative sample was analyzed to determine the difference in FeNO levels between patients with ACOS and those with COPD alone in the US population.
This is a cross-sectional analysis of the National Health and Nutrition Examination Survey from 2007 through 2012. All subjects aged ≥40 years with COPD were identified. ACOS was defined as self-reported wheezing in past 12 months plus bronchodilator response (forced expiratory volume increase of >200 mL and >12%) or self-reported physician diagnosis of asthma.
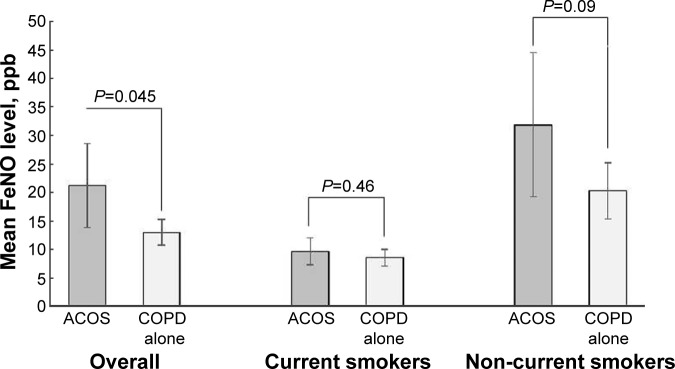
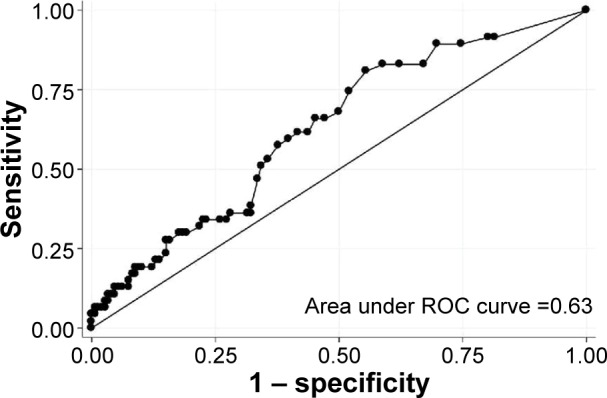
A total of 197 subjects with COPD were identified in the National Health and Nutrition Examination Survey. Of these, 23% met the criteria of ACOS. The FeNO level was higher in subjects with ACOS compared with those with COPD alone in both unadjusted (mean 21.2 ppb vs 13.0 ppb; difference, 8.2 [95% CI, 0.2 to 16.2]; =0.045) and adjusted (difference, 8.2 [95% CI, 0.9 to 15.5]; =0.03) analyses. Although there was no significant difference among current smokers, the FeNO level was significantly higher in non-current smokers with ACOS than nonsmokers with COPD alone (mean 31.9 ppb vs 20.3 ppb; adjusted difference, 20.5 [95% CI, 4.4 to 36.6]; =0.02). In a sensitivity analysis using an alternative definition of ACOS, the results did not change materially. The diagnostic value of FeNO to discriminate ACOS from COPD alone was not sufficient, with the area under the curve of 0.63 (95% CI, 0.54 to 0.72).
By using nationally representative US data, it was found that 23% of COPD subjects met the ACOS criteria and also that the FeNO level was higher in subjects with ACOS compared with those with COPD alone, particularly in non-current smokers.
近期研究提出哮喘-慢性阻塞性肺疾病(COPD)重叠综合征(ACOS)患者存在T2介导的炎症。然而,关于ACOS患者与单纯COPD患者的呼出气一氧化氮分数(FeNO)是否存在差异,目前所知甚少。为填补这一知识空白,我们对一个具有全国代表性的样本进行了分析,以确定美国人群中ACOS患者与单纯COPD患者FeNO水平的差异。
这是一项对2007年至2012年美国国家健康与营养检查调查的横断面分析。确定了所有年龄≥40岁的COPD患者。ACOS被定义为过去12个月内自我报告的喘息加上支气管扩张剂反应(用力呼气量增加>200 mL且>12%)或自我报告医生诊断为哮喘。
在美国国家健康与营养检查调查中,共确定了197例COPD患者。其中,23%符合ACOS标准。在未调整分析(平均21.2 ppb对13.0 ppb;差异,8.2 [95% CI,0.2至16.2];P = 0.045)和调整分析(差异,8.2 [95% CI,0.9至15.5];P = 0.03)中,ACOS患者的FeNO水平均高于单纯COPD患者。虽然当前吸烟者之间无显著差异,但非当前吸烟的ACOS患者的FeNO水平显著高于单纯COPD的非吸烟者(平均31.9 ppb对20.3 ppb;调整后差异,20.5 [95% CI,4.4至36.6];P = 0.02)。在使用ACOS替代定义的敏感性分析中,结果没有实质性变化。FeNO区分ACOS与单纯COPD的诊断价值不足,曲线下面积为0.63(95% CI,0.54至0.72)。
通过使用具有全国代表性的美国数据,发现23%的COPD患者符合ACOS标准,且ACOS患者的FeNO水平高于单纯COPD患者,尤其是在非当前吸烟者中。