Department of Epidemiology and Public Health, University College London and UK Centre for Tobacco and Alcohol Studies, London, UK.
School of Health Sciences, University of Stirling and UK Centre for Tobacco and Alcohol Studies, Stirling, UK.
Nicotine Tob Res. 2017 Dec 13;20(1):81-88. doi: 10.1093/ntr/ntw258.
Nicotine replacement therapy (NRT) was licensed for harm reduction in the United Kingdom in 2005, and guidance to UK Stop-Smoking Services (SSS) to include long-term partial or complete substitution of cigarettes with NRT was issued in 2013. Yet, NRT prevalence data and data on changes in biomarkers associated with long-term NRT use among SSS clients are scarce.
SSS clients abstinent 4 weeks postquit date were followed up at 12 months. At baseline standard sociodemographic, smoking and SSS use characteristics were collected and of those eligible, 60.6% (1047/1728) provided data on smoking status and NRT use at follow-up. A subsample also provided saliva samples at baseline and of those eligible, 36.2% (258/712) provided follow-up samples. Saliva was analyzed for cotinine (a metabolite of nicotine) and alpha-amylase (a stress biomarker).
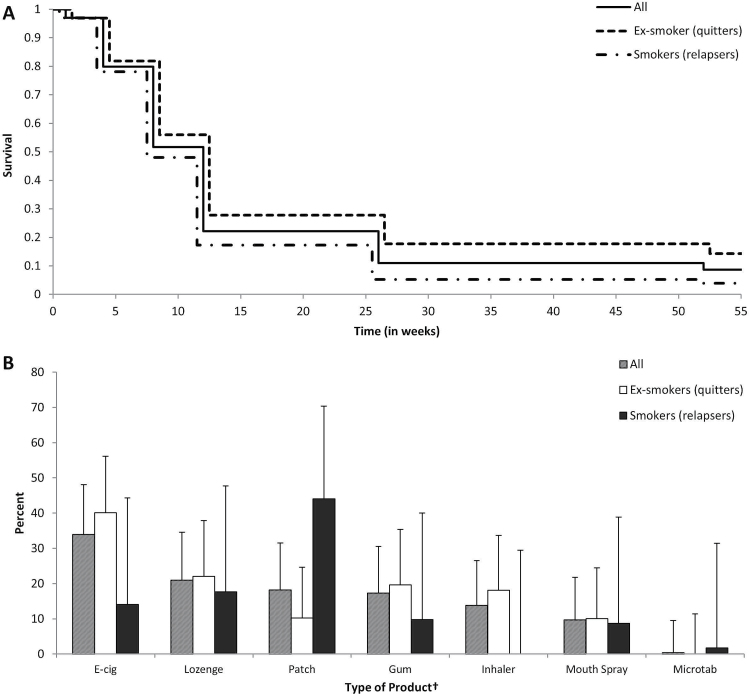
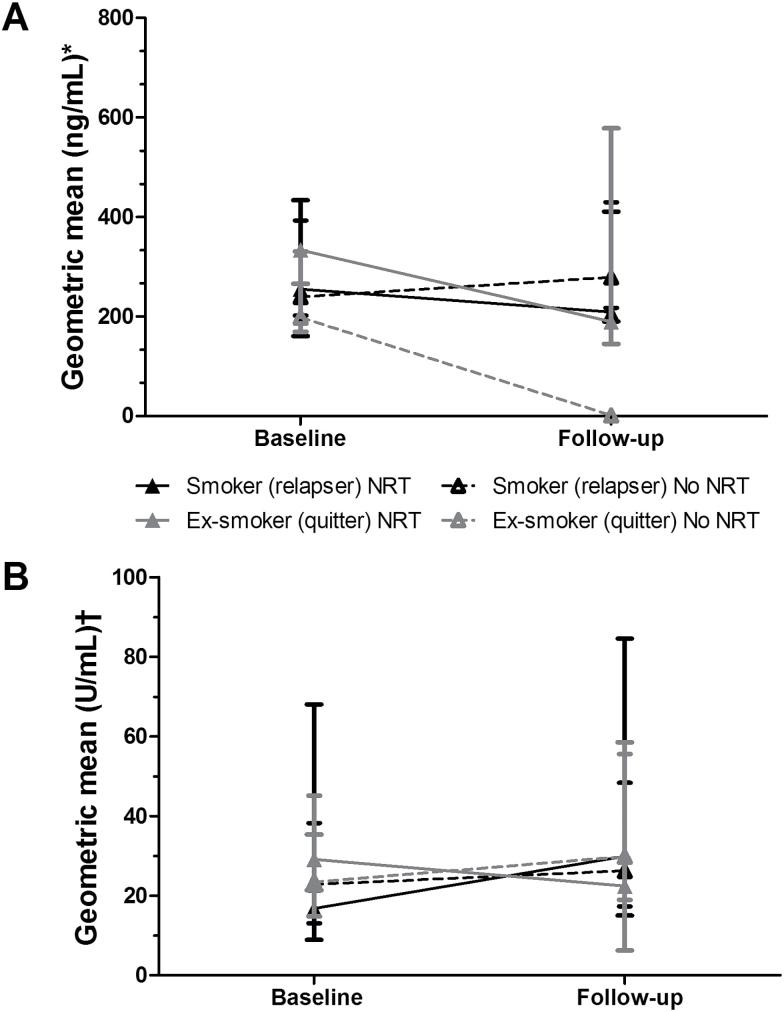
Among those who had used NRT during their initial quit attempt (61.5%, 95% CI 58.4%-64.6%), 6.0% (95% CI 4.3%-8.3%) were still using NRT at 1 year, significantly more ex-smokers than relapsed smokers (9.5% vs. 3.7%; p = .005). In adjusted analysis, NRT use interacted with smoking status to determine change in cotinine, but not alpha-amylase, levels (Wald χ2 (1) = 13.0, p < .001): cotinine levels remained unchanged in relapsed smokers and ex-smokers with long-term NRT use but decreased in ex-smokers without long-term NRT use.
Long-term NRT use is uncommon in SSS clients, particularly among relapsed smokers. Its use is associated with continued high intake of nicotine among ex-smokers but does not increase nicotine intake in smokers. It does not appear to affect stress response.
Little is known about the long-term effects of NRT. Given an increasing shift towards harm reduction in tobacco control, reducing the harm from combustible products by partial or complete substitution with noncombustible products, more data on long-term use are needed. This study shows that in the context of SSS, clients rarely use products for up to a year and that NRT use does not affect users' stress response. Ex-smokers using NRT long-term can completely replace nicotine from cigarettes with nicotine from NRT; long-term NRT use by continuing smokers does not increase nicotine intake. Long-term NRT appears to be a safe and effective way to reduce exposure to combustible nicotine.
尼古丁替代疗法(NRT)于 2005 年在英国获得减少危害许可证,2013 年发布的英国戒烟服务(SSS)指南建议长期部分或完全用 NRT 替代香烟。然而,关于 SSS 客户中 NRT 使用率的流行数据和与长期 NRT 使用相关的生物标志物变化的数据却很少。
SSS 客户在戒烟 4 周后进行随访,随访时间为 12 个月。在基线时收集了标准的社会人口统计学、吸烟和 SSS 使用特征,并对符合条件的 60.6%(1047/1728)的参与者在随访时提供了吸烟状况和 NRT 使用的数据。亚组还在基线时提供了唾液样本,其中符合条件的 36.2%(258/712)提供了随访样本。对唾液中的可替宁(尼古丁的代谢物)和α-淀粉酶(一种应激生物标志物)进行了分析。
在最初的戒烟尝试中使用过 NRT 的参与者中(61.5%,95%CI 58.4%-64.6%),6.0%(95%CI 4.3%-8.3%)在 1 年内仍在使用 NRT,显著高于复吸者(9.5%比 3.7%;p =.005)。在调整分析中,NRT 使用与吸烟状况相互作用,决定了可替宁水平的变化,但不影响α-淀粉酶水平(Wald χ2(1)= 13.0,p <.001):在长期使用 NRT 的复吸者和戒烟者中,可替宁水平保持不变,但在未长期使用 NRT 的戒烟者中,可替宁水平下降。
在 SSS 客户中,长期使用 NRT 并不常见,特别是在复吸者中。它的使用与戒烟者中尼古丁的持续高摄入量有关,但不会增加吸烟者的尼古丁摄入量。它似乎不会影响应激反应。
关于 NRT 的长期影响知之甚少。鉴于在烟草控制中越来越倾向于减少危害,通过部分或完全用非燃烧产品替代燃烧产品来减少燃烧产品的危害,需要更多关于长期使用的数据。本研究表明,在 SSS 背景下,客户很少使用产品长达一年,并且 NRT 使用不会影响用户的应激反应。长期使用 NRT 的戒烟者可以用 NRT 中的尼古丁完全替代香烟中的尼古丁;持续吸烟者长期使用 NRT 不会增加尼古丁摄入量。长期使用 NRT 似乎是一种安全有效的减少接触可燃尼古丁的方法。