Opotowsky Alexander R, Baraona Fernando R, Mc Causland Finnian R, Loukas Brittani, Landzberg Elizabeth, Landzberg Michael J, Sabbisetti Venkata, Waikar Sushrut S
Department of Cardiology, Boston Children's Hospital, Boston, Massachusetts, USA.
Department of Medicine, Brigham and Women's Hospital, Boston, Massachusetts, USA.
Heart. 2017 Mar;103(6):434-442. doi: 10.1136/heartjnl-2016-309729. Epub 2016 Sep 26.
To define whether adults with a Fontan circulation, who have lifelong venous congestion and limited cardiac output, have impaired glomerular filtration rate (GFR) or elevated urinary biomarkers of kidney injury.
We measured circulating cystatin C and creatinine (n=70) and urinary creatinine, albumin, kidney injury molecule-1 (KIM-1), neutrophil gelatinase-associated lipocalin (NGAL) and N-acetyl glucosaminidase (NAG) (n=59) in ambulatory adult Fontan patients and 20 age-matched and sex-matched controls. Urinary biomarkers were normalised to urine creatinine concentration. Survival free from non-elective cardiovascular hospitalisation was compared by estimated GFR and urinary biomarker levels using survival analysis.
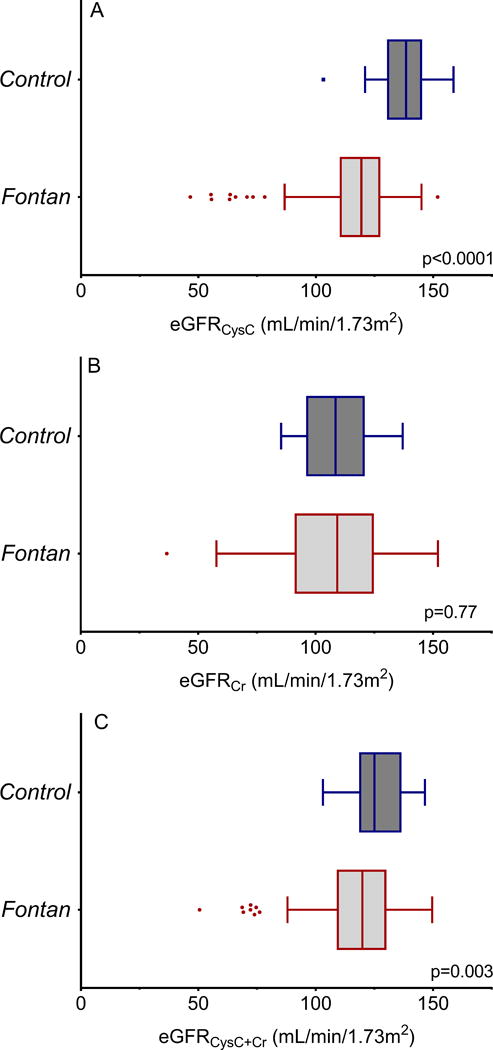
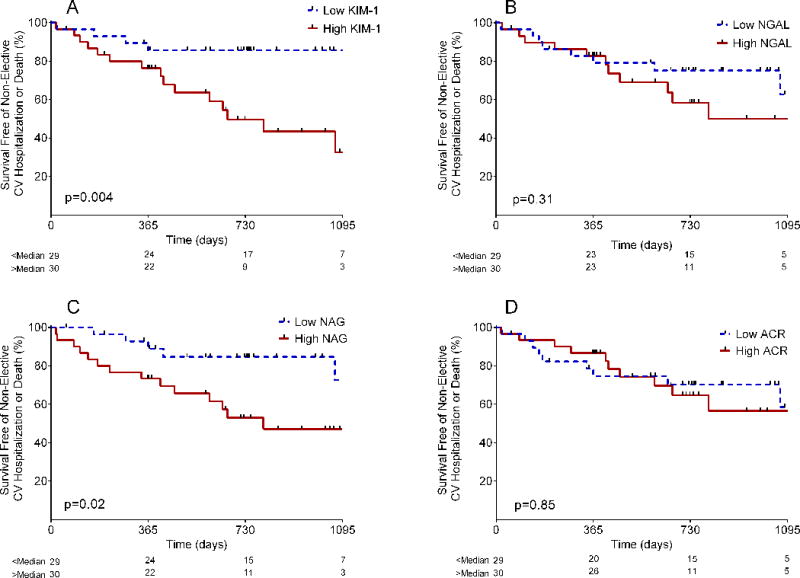
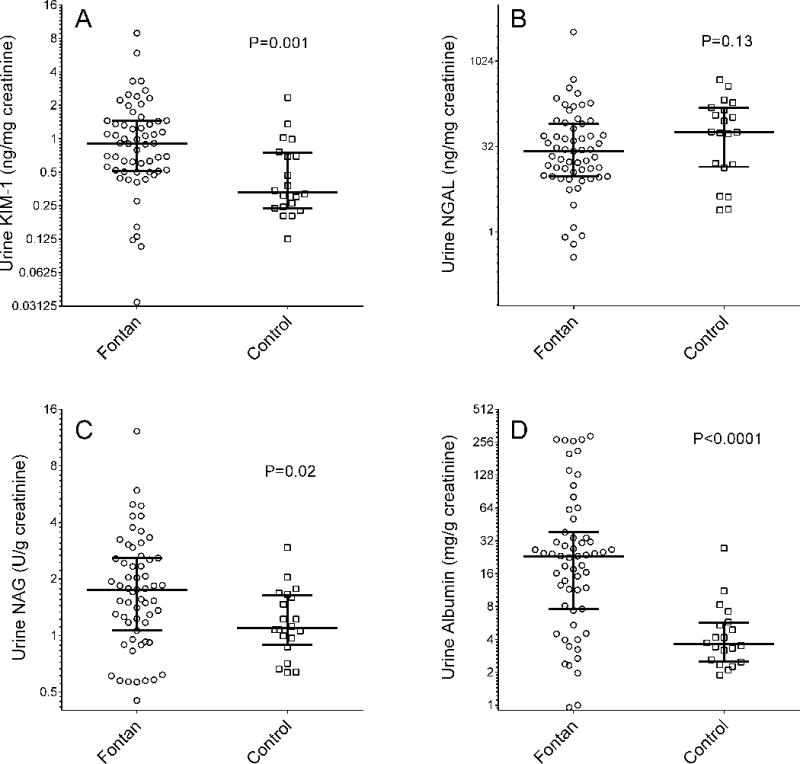
Cystatin C GFR was lower in the Fontan group compared with controls (114.2±22.8 vs 136.3±12.8 mL/min/1.73 m, p<0.0001); GFR<90 mL/min/1.73 m in 14.3% vs 0% of controls. Albumin-to-creatinine ratio (ACR), KIM-1 and NAG were elevated compared with controls; ACR=23.2 (7.6-38.3) vs 3.6 (2.5-5.7) mg/g, p<0.0001; NAG=1.8 (1.1-2.6) vs 1.1 (0.9-1.6) U/g, p=0.02; KIM-1=0.91 (0.52-1.45) vs 0.33 (0.24-0.74) ng/mg, p=0.001. Microalbuminuria, ACR>30 mg/g, was present in 33.9% of the Fontan patients but in none of the controls. Over median 707 (IQR 371-942)-day follow-up, 31.4% of patients had a clinical event. Higher KIM-1 and NAG were associated with higher risk of non-elective hospitalisation or death (HR/+1 SD=2.1, 95% CI 1.3 to 3.3, p=0.002; HR/+1 SD=1.6, 95% CI 1.05 to 2.4, p=0.03, respectively); cystatin C GFR was associated with risk of the outcome (HR/+1 SD=0.66, 95% CI 0.48 to 0.90, p=0.009) but creatinine-based GFR was not (HR/+1 SD=0.91, 95% CI 0.61 to 1.38, p=0.66). Neither ACR nor NGAL was associated with events.
The Fontan circulation is commonly associated with reduced estimated GFR and evidence for glomerular and tubular injury. Those with lower cystatin C GFR and tubular injury are at increased risk of adverse outcomes.
确定患有Fontan循环的成年人,他们终生存在静脉淤血且心输出量有限,是否存在肾小球滤过率(GFR)受损或肾脏损伤的尿生物标志物升高。
我们测量了门诊成年Fontan患者以及20名年龄和性别匹配的对照者的循环胱抑素C和肌酐(n = 70),以及尿肌酐、白蛋白、肾损伤分子-1(KIM-1)、中性粒细胞明胶酶相关脂质运载蛋白(NGAL)和N-乙酰氨基葡萄糖苷酶(NAG)(n = 59)。尿生物标志物以尿肌酐浓度进行标准化。使用生存分析,通过估计的GFR和尿生物标志物水平比较无非择期心血管住院的生存率。
Fontan组的胱抑素C GFR低于对照组(114.2±22.8 vs 136.3±12.8 mL/min/1.73 m²,p<0.0001);GFR<90 mL/min/1.73 m²的患者在Fontan组中占14.3%,而对照组中为0%。与对照组相比,白蛋白与肌酐比值(ACR)、KIM-1和NAG升高;ACR = 23.2(7.6 - 38.3)vs 3.6(2.5 - 5.7)mg/g,p<0.0001;NAG = 1.8(1.1 - 2.6)vs 1.1(0.9 - 1.6)U/g,p = 0.02;KIM-1 = 0.91(0.52 - 1.45)vs 0.33(0.24 - 0.74)ng/mg,p = 0.001。微量白蛋白尿,即ACR>30 mg/g,在33.9%的Fontan患者中存在,而对照组中无一例出现。在中位707(IQR 371 - 942)天的随访中,31.4%的患者发生了临床事件。较高的KIM-1和NAG与非择期住院或死亡的较高风险相关(HR/+1 SD =