Kim Hanna, Sanchez Gina A Montealegre, Goldbach-Mansky Raphaela
Lawrence Shulman Scholar in Translational Research, Pediatric Translational Research Branch, National Institute of Arthritis Musculoskeletal and Skin Diseases (NIAMS), National Institutes of Health (NIH), Bethesda, MD, USA.
Translational Autoinflammatory Disease Studies, National Institute of Allergy and Infectious Diseases (NIAID), and NIAMS, National Institutes of Health (NIH), Bethesda, MD, USA.
J Mol Med (Berl). 2016 Oct;94(10):1111-1127. doi: 10.1007/s00109-016-1465-5. Epub 2016 Sep 27.
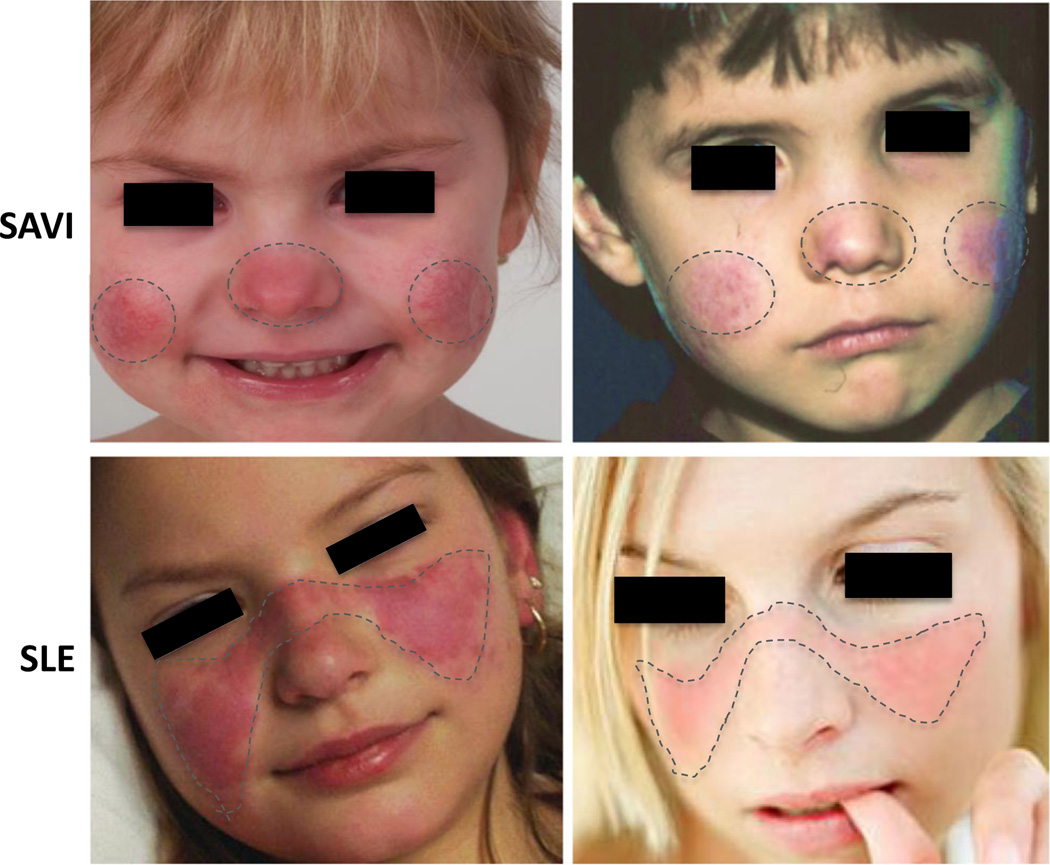
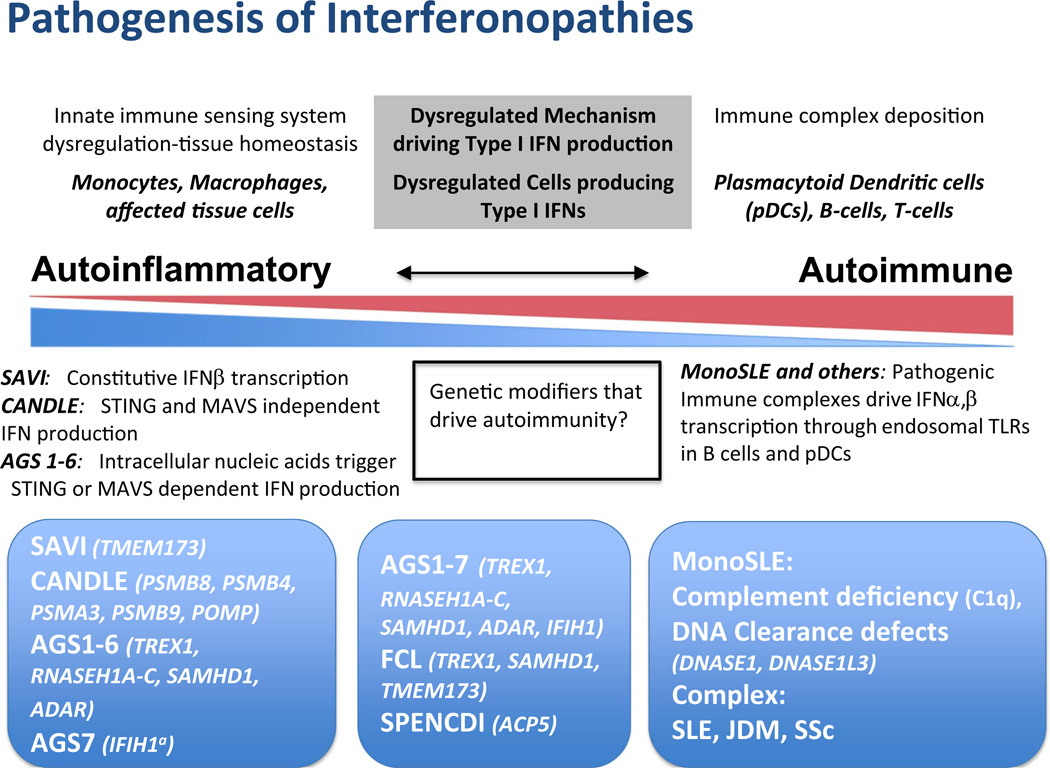
Autoinflammatory disorders are sterile inflammatory conditions characterized by episodes of early-onset fever and disease-specific patterns of organ inflammation. Recently, the discoveries of monogenic disorders with strong type I interferon (IFN) signatures caused by mutations in proteasome degradation and cytoplasmic RNA and DNA sensing pathways suggest a pathogenic role of IFNs in causing autoinflammatory phenotypes. The IFN response gene signature (IGS) has been associated with systemic lupus erythematosus (SLE) and other autoimmune diseases. In this review, we compare the clinical presentations and pathogenesis of two IFN-mediated autoinflammatory diseases, CANDLE and SAVI, with Aicardi Goutières syndrome (AGS) and monogenic forms of SLE (monoSLE) caused by loss-of-function mutations in complement 1 (C1q) or the DNA nucleases, DNASE1 and DNASE1L3. We outline differences in intracellular signaling pathways that fuel a pathologic type I IFN amplification cycle. While IFN amplification is caused by predominantly innate immune cell dysfunction in SAVI, CANDLE, and AGS, autoantibodies to modified RNA and DNA antigens interact with tissues and immune cells including neutrophils and contribute to IFN upregulation in some SLE patients including monoSLE, thus justifying a grouping of "autoinflammatory" and "autoimmune" interferonopathies. Understanding of the differences in the cellular sources and signaling pathways will guide new drug development and the use of emerging targeted therapies.
自身炎症性疾病是一类无菌性炎症状态,其特征为早发性发热发作以及特定疾病的器官炎症模式。最近,由蛋白酶体降解以及细胞质RNA和DNA传感途径中的突变所导致的具有强烈I型干扰素(IFN)特征的单基因疾病的发现,提示了IFN在引发自身炎症表型中的致病作用。IFN反应基因特征(IGS)已与系统性红斑狼疮(SLE)及其他自身免疫性疾病相关联。在本综述中,我们比较了两种IFN介导的自身炎症性疾病——慢性非典型中性粒细胞皮肤病伴脂膜炎样皮疹、嗜中性粒细胞增多及皮下脂膜炎样T细胞淋巴瘤(CANDLE)和干扰素基因刺激因子(STING)相关血管病伴婴儿期发病(SAVI)——与由补体1(C1q)或DNA核酸酶DNASE1和DNASE1L3功能丧失突变引起的艾卡迪-古铁雷斯综合征(AGS)和单基因形式的SLE(单基因SLE)的临床表现和发病机制。我们概述了促成病理性I型IFN扩增循环的细胞内信号通路的差异。虽然在SAVI、CANDLE和AGS中,IFN扩增主要由先天性免疫细胞功能障碍引起,但针对修饰的RNA和DNA抗原的自身抗体与包括中性粒细胞在内的组织和免疫细胞相互作用,并在包括单基因SLE在内的一些SLE患者中促成IFN上调,因此证明了“自身炎症性”和“自身免疫性”干扰素病的分组是合理的。了解细胞来源和信号通路的差异将指导新药开发以及新兴靶向治疗的应用。