Seo Young-Seok, Kim Mi-Sook, Yoo Hyung-Jun, Jang Won Il, Paik Eun Kyung, Han Chul Ju, Lee Byung-Hee
Department of Radiation Oncology, Korea Institute of Radiological & Medical Sciences, Seoul, Korea.
Department of Internal Medicine, Korea Institute of Radiological & Medical Sciences, Seoul, Korea.
Cancer Med. 2016 Nov;5(11):3094-3101. doi: 10.1002/cam4.893. Epub 2016 Oct 5.
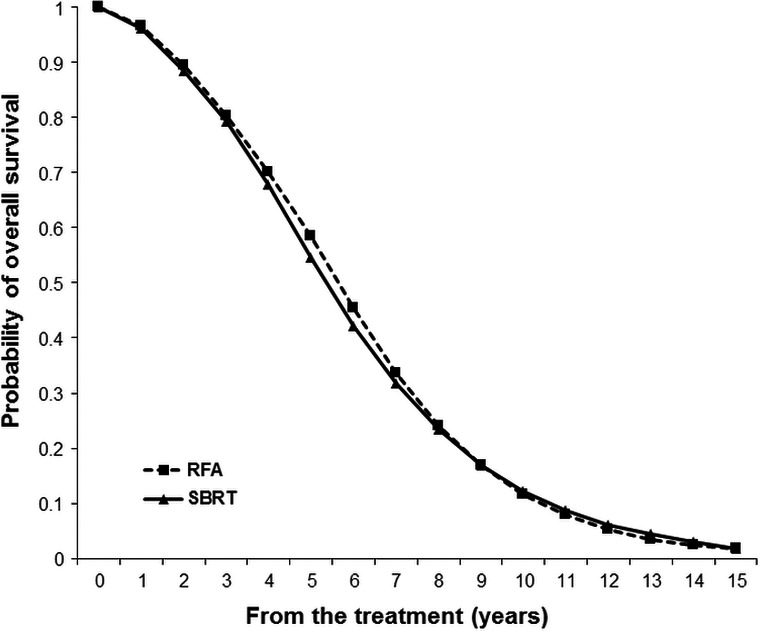
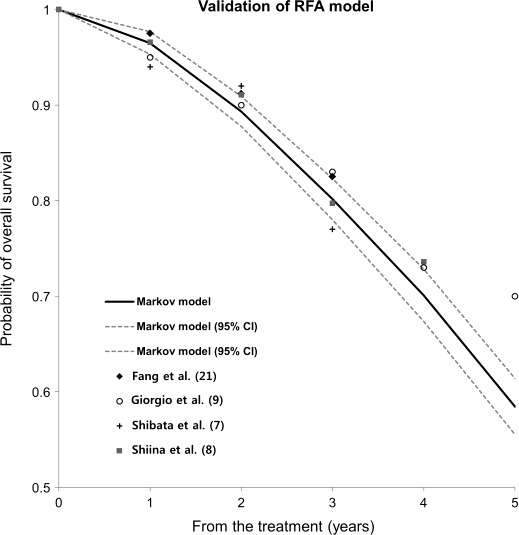
The aim of this study is to compare radiofrequency ablation (RFA) with stereotactic body radiotherapy (SBRT) for hepatocellular carcinomas (HCC) smaller than 3 cm. A Markov cohort model was developed to simulate a cohort of patients aged 60-65 years with small HCCs who had undergone either RFA or SBRT and were followed up over their remaining life expectancy. The inclusion criteria were: (1) HCC ≤3 cm in diameter with ≤ 3 nodules; (2) absence of extrahepatic metastasis or portal/hepatic vein invasion; (3) Child-Pugh Class A or B. Twenty thousand virtual patients were randomly assigned to undergo RFA or SBRT. Predicted life expectancy was 6.452 and 6.371 years in the RFA and SBRT groups, respectively. The probability distributions of the expected overall survival were nearly identical. The 95% confidence intervals were 6.25-6.66 and 6.17-6.58 years for RFA and SBRT, respectively. The difference between RFA and SBRT was insignificant (P = 0.2884). Two-way sensitivity analysis demonstrated that if the tumor is 2-3 cm, SBRT is the preferred treatment option. Our Markov model has shown that expected overall survival of SBRT is nearly identical to RFA in HCCs smaller than 3 cm, but SBRT may have an advantage for tumors 2 cm and larger. A randomized trial is required to confirm these findings.
本研究旨在比较射频消融(RFA)与立体定向体部放疗(SBRT)治疗直径小于3cm的肝细胞癌(HCC)的效果。构建了一个马尔可夫队列模型,以模拟一组年龄在60 - 65岁之间、患有小肝癌且接受过RFA或SBRT治疗并在其剩余预期寿命内接受随访的患者队列。纳入标准为:(1)直径≤3cm且结节数≤3个的HCC;(2)无肝外转移或门静脉/肝静脉侵犯;(3)Child-Pugh A或B级。20000名虚拟患者被随机分配接受RFA或SBRT治疗。RFA组和SBRT组的预测预期寿命分别为6.452年和6.371年。预期总生存的概率分布几乎相同。RFA组和SBRT组的95%置信区间分别为6.25 - 6.66年和6.17 - 6.58年。RFA和SBRT之间的差异不显著(P = 0.2884)。双向敏感性分析表明,如果肿瘤为2 - 3cm,SBRT是首选治疗方案。我们的马尔可夫模型表明,对于直径小于3cm的HCC,SBRT的预期总生存与RFA几乎相同,但对于2cm及以上的肿瘤SBRT可能具有优势。需要进行一项随机试验来证实这些发现。