Bouza C, Lopez-Cuadrado T, Amate-Blanco J M
Health-Care Technology Assessment Agency, Institute of Health Carlos III, Madrid, Spain.
National Centre of Epidemiology, Institute of Health Carlos III, Madrid, Spain.
Crit Care. 2016 Oct 3;20(1):313. doi: 10.1186/s13054-016-1497-9.
Severe sepsis is a challenge for healthcare systems, and epidemiological studies are essential to assess its burden and trends. However, there is no consensus on which coding strategy should be used to reliably identify severe sepsis. This study assesses the use of explicit codes to define severe sepsis and the impacts of this on the incidence and in-hospital mortality rates.
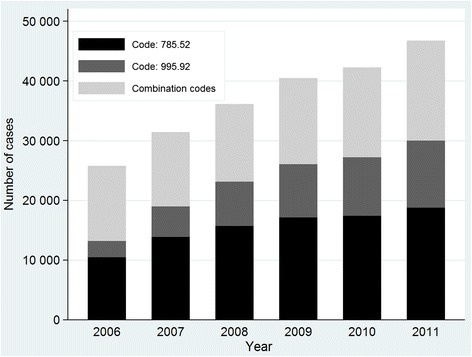
We examined episodes of severe sepsis in adults aged ≥18 years registered in the 2006-2011 national hospital discharge database, identified in an exclusive manner by two ICD-9-CM coding strategies: (1) those assigned explicit ICD-9-CM codes (995.92, 785.52); and (2) those assigned combined ICD-9-CM infection and organ dysfunction codes according to modified Martin criteria. The coding strategies were compared in terms of the populations they defined and their relative implementation. Trends were assessed using Joinpoint regression models and expressed as annual percentage change (APC).
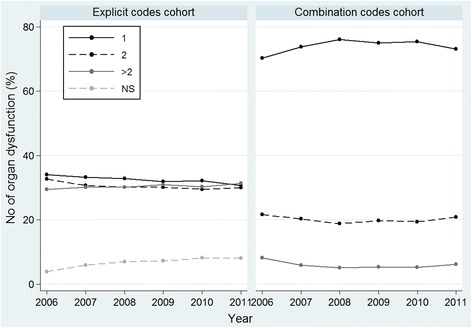
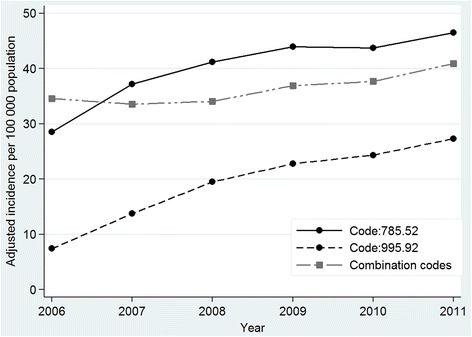
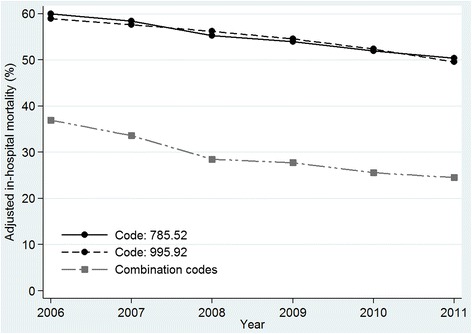
Of 222 846 episodes of severe sepsis identified, 138 517 (62.2 %) were assigned explicit codes and 84 329 (37.8 %) combination codes; incidence rates were 60.6 and 36.9 cases per 100 000 inhabitants, respectively. Despite similar demographic characteristics, cases identified by explicit codes involved fewer comorbidities, fewer registered pathogens, greater extent of organ dysfunction (two or more organs affected in 60 % versus 26 % of cases) and higher in-hospital mortality (54.5 % versus 29 %; risk ratio 1.86, 95 % CI 1.83, 1.88). Between 2006 and 2011, explicit codes were increasingly implemented. Standardised incidence rates in this cohort increased over time with an APC of 12.3 % (95 % CI 4.4, 20.8); in the combination code cohort, rates increased by 3.8 % (95 % CI 1.3, 6.3). A decreasing trend in mortality was observed in both cohorts though the APC was -8.1 % (95 % CI -10.4, -5.7) in the combination code cohort and -3.5 % (95 % CI -3.9, -3.2) in the explicit code cohort.
Our findings suggest greater and increasing use of explicit codes for adult severe sepsis in Spain. This trend will have substantial impacts on epidemiological estimates, because these codes capture cases featuring greater organ dysfunction and in-hospital mortality.
严重脓毒症是医疗系统面临的一项挑战,流行病学研究对于评估其负担和趋势至关重要。然而,对于应采用哪种编码策略来可靠识别严重脓毒症,目前尚无共识。本研究评估了使用明确编码来定义严重脓毒症及其对发病率和院内死亡率的影响。
我们检查了2006 - 2011年国家医院出院数据库中登记的≥18岁成年人的严重脓毒症病例,通过两种ICD - 9 - CM编码策略以排他方式识别:(1)那些被分配明确ICD - 9 - CM编码(995.92、785.52)的病例;(2)那些根据改良马丁标准被分配ICD - 9 - CM感染和器官功能障碍组合编码的病例。比较了这两种编码策略所定义的人群及其相对实施情况。使用Joinpoint回归模型评估趋势,并表示为年度百分比变化(APC)。
在识别出的222846例严重脓毒症病例中,138517例(62.2%)被分配了明确编码,84329例(37.8%)被分配了组合编码;发病率分别为每10万居民60.6例和每10万居民36.9例。尽管人口统计学特征相似,但通过明确编码识别出的病例合并症较少,登记的病原体较少,器官功能障碍程度更高(60%的病例有两个或更多器官受影响,而组合编码病例中这一比例为26%),且院内死亡率更高(54.5%对29%;风险比1.86,95%CI 1.83,1.88)。2006年至2011年期间,明确编码的使用越来越多。该队列中的标准化发病率随时间增加,APC为12.3%(95%CI 4.4,20.8);在组合编码队列中,发病率增加了3.8%(9%CI 1.3,6.3)。两个队列中均观察到死亡率呈下降趋势,不过组合编码队列中的APC为 - 8.1%(95%CI - 10.4, - 5.7),明确编码队列中的APC为 - 3.5%(95%CI - 3.9, - 3.2)。
我们的研究结果表明,在西班牙,成人严重脓毒症使用明确编码的情况越来越多且使用程度更高。这一趋势将对流行病学估计产生重大影响,因为这些编码涵盖了器官功能障碍更严重和院内死亡率更高的病例。