Casarotto Silvia, Comanducci Angela, Rosanova Mario, Sarasso Simone, Fecchio Matteo, Napolitani Martino, Pigorini Andrea, G Casali Adenauer, Trimarchi Pietro D, Boly Melanie, Gosseries Olivia, Bodart Olivier, Curto Francesco, Landi Cristina, Mariotti Maurizio, Devalle Guya, Laureys Steven, Tononi Giulio, Massimini Marcello
Department of Biomedical and Clinical Sciences "L. Sacco", University of Milan, Milan, Italy.
Fondazione Europea per la Ricerca Biomedica, Milan, Italy.
Ann Neurol. 2016 Nov;80(5):718-729. doi: 10.1002/ana.24779. Epub 2016 Nov 2.
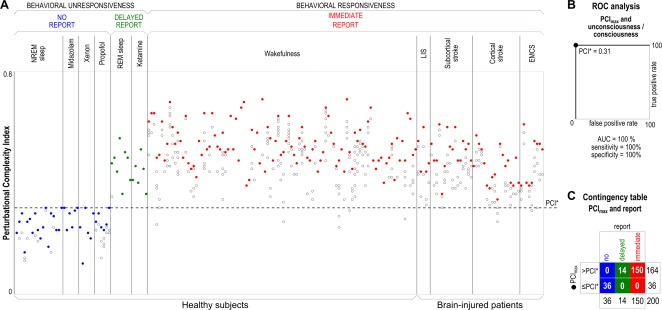
Validating objective, brain-based indices of consciousness in behaviorally unresponsive patients represents a challenge due to the impossibility of obtaining independent evidence through subjective reports. Here we address this problem by first validating a promising metric of consciousness-the Perturbational Complexity Index (PCI)-in a benchmark population who could confirm the presence or absence of consciousness through subjective reports, and then applying the same index to patients with disorders of consciousness (DOCs).
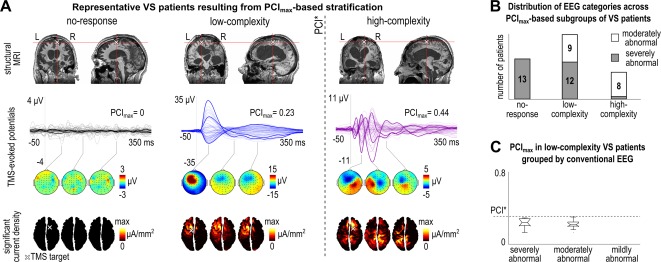
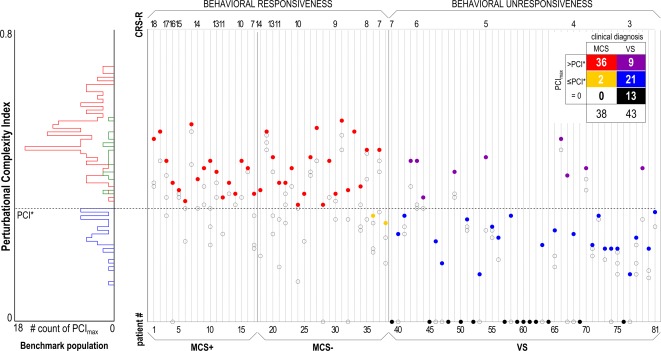
The benchmark population encompassed 150 healthy controls and communicative brain-injured subjects in various states of conscious wakefulness, disconnected consciousness, and unconsciousness. Receiver operating characteristic curve analysis was performed to define an optimal cutoff for discriminating between the conscious and unconscious conditions. This cutoff was then applied to a cohort of noncommunicative DOC patients (38 in a minimally conscious state [MCS] and 43 in a vegetative state [VS]).
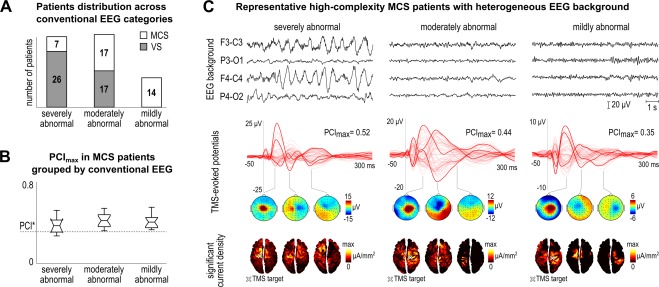
We found an empirical cutoff that discriminated with 100% sensitivity and specificity between the conscious and the unconscious conditions in the benchmark population. This cutoff resulted in a sensitivity of 94.7% in detecting MCS and allowed the identification of a number of unresponsive VS patients (9 of 43) with high values of PCI, overlapping with the distribution of the benchmark conscious condition.
Given its high sensitivity and specificity in the benchmark and MCS population, PCI offers a reliable, independently validated stratification of unresponsive patients that has important physiopathological and therapeutic implications. In particular, the high-PCI subgroup of VS patients may retain a capacity for consciousness that is not expressed in behavior. Ann Neurol 2016;80:718-729.
由于无法通过主观报告获得独立证据,因此在行为无反应的患者中验证基于大脑的客观意识指标是一项挑战。在此,我们通过以下方式解决这一问题:首先在一个可以通过主观报告确认意识存在与否的基准人群中验证一种有前景的意识指标——微扰复杂性指数(PCI),然后将相同指标应用于意识障碍(DOC)患者。
基准人群包括150名健康对照者以及处于不同意识清醒状态、分离意识状态和无意识状态的可交流脑损伤受试者。进行受试者操作特征曲线分析以确定区分有意识和无意识状态的最佳临界值。然后将此临界值应用于一组无法交流的DOC患者(38例处于最低意识状态[MCS],43例处于植物状态[VS])。
我们发现了一个经验临界值,该临界值在基准人群中区分有意识和无意识状态时具有100%的敏感性和特异性。此临界值在检测MCS时的敏感性为94.7%,并能识别出一些PCI值较高的无反应VS患者(43例中有9例),其PCI值分布与基准有意识状态重叠。
鉴于PCI在基准人群和MCS人群中具有高敏感性和特异性,它为无反应患者提供了一种可靠的、经过独立验证的分层方法,具有重要的生理病理学和治疗意义。特别是,VS患者中PCI值高的亚组可能保留了一种未在行为中表现出来的意识能力。《神经病学纪事》2016年;80:718 - 729。