Metroplex Clinical Research Center, Dallas, Texas.
University of Colorado, Denver.
Arthritis Rheumatol. 2017 Mar;69(3):506-517. doi: 10.1002/art.39953.
We undertook this phase III study to evaluate baricitinib, an orally administered JAK-1/JAK-2 inhibitor, as monotherapy or combined with methotrexate (MTX) compared to MTX monotherapy in patients with active rheumatoid arthritis (RA) who had received no or minimal conventional synthetic disease-modifying antirheumatic drugs (DMARDs) and who were naive to biologic DMARDs.
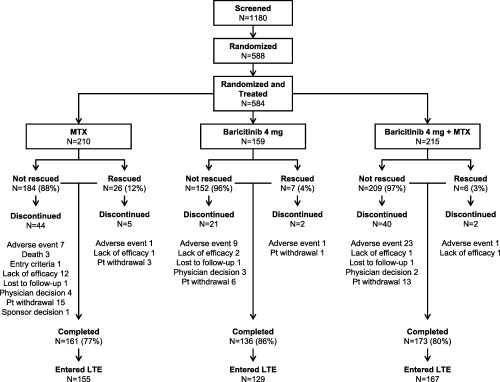
A total of 588 patients were randomized 4:3:4 to receive MTX monotherapy (once weekly), baricitinib monotherapy (4 mg once daily), or the combination of baricitinib and MTX for 52 weeks. The primary end point assessment was a noninferiority comparison of baricitinib monotherapy to MTX monotherapy based on the proportion of patients meeting the American College of Rheumatology 20% improvement criteria (achieving an ACR20 response) at week 24.
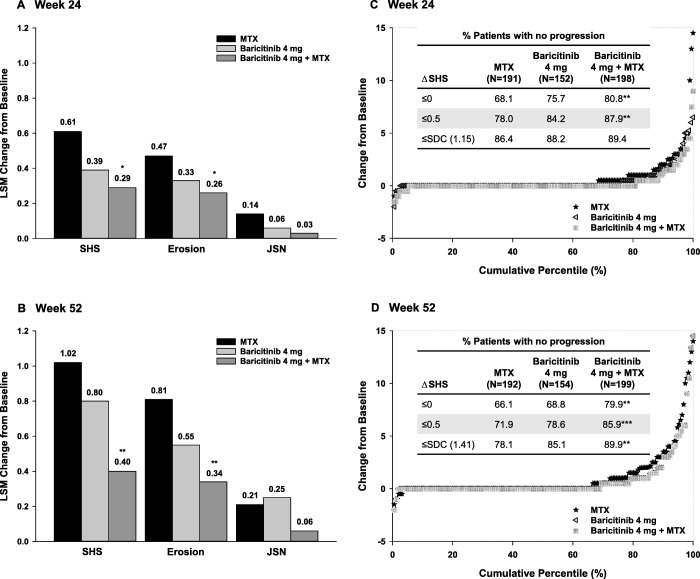
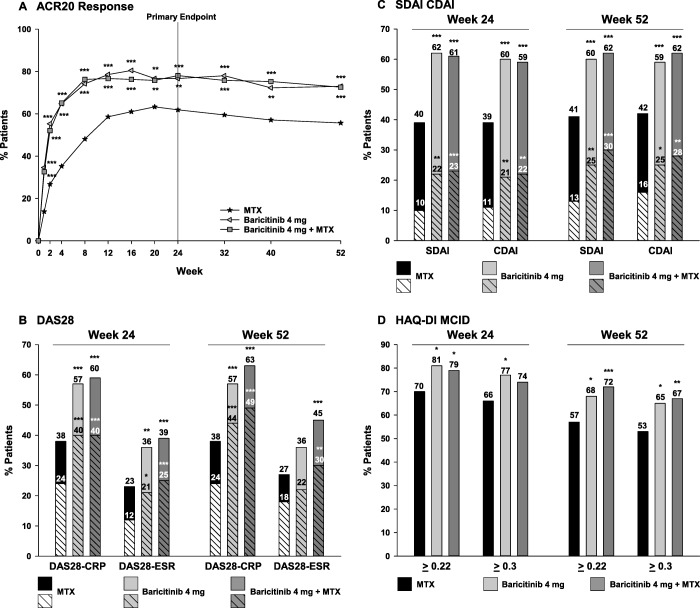
The study met its primary objective. Moreover, baricitinib monotherapy was found to be superior to MTX monotherapy at week 24, with a higher ACR20 response rate (77% versus 62%; P ≤ 0.01). Similar results were observed for combination therapy. Compared to MTX monotherapy, significant improvements in disease activity and physical function were observed for both baricitinib groups as early as week 1. Radiographic progression was reduced in both baricitinib groups compared to MTX monotherapy; the difference was statistically significant for baricitinib plus MTX. The rates of serious adverse events (AEs) were similar across treatment groups, while rates of some treatment-emergent AEs, including infections, were increased with baricitinib plus MTX. Three deaths were reported, all occurring in the MTX monotherapy group. Malignancies, including nonmelanoma skin cancer, were reported in 1 patient receiving MTX monotherapy, 1 receiving baricitinib monotherapy, and 4 receiving baricitinib plus MTX.
Baricitinib alone or in combination with MTX demonstrated superior efficacy with acceptable safety compared to MTX monotherapy as initial therapy for patients with active RA.
我们进行这项 III 期研究,旨在评估巴利昔替尼,一种口服 JAK-1/JAK-2 抑制剂,与甲氨蝶呤(MTX)单药治疗或联合治疗相比,在接受过最少的传统合成疾病修饰抗风湿药物(DMARDs)且对生物 DMARDs 无经验的活动性类风湿关节炎(RA)患者中作为单药治疗或联合治疗。
共有 588 名患者被随机分为 4:3:4 组,分别接受 MTX 单药治疗(每周一次)、巴利昔替尼单药治疗(4 mg 每日一次)或巴利昔替尼联合 MTX 治疗 52 周。主要终点评估是基于 24 周时达到美国风湿病学会 20%改善标准(实现 ACR20 应答)的患者比例,对巴利昔替尼单药与 MTX 单药进行非劣效性比较。
该研究达到了主要目标。此外,在第 24 周时,巴利昔替尼单药治疗的疗效优于 MTX 单药治疗,ACR20 应答率更高(77% vs. 62%;P ≤ 0.01)。联合治疗也观察到类似的结果。与 MTX 单药治疗相比,巴利昔替尼组在第 1 周就观察到疾病活动度和身体功能的显著改善。与 MTX 单药治疗相比,巴利昔替尼组的放射学进展均减少,巴利昔替尼联合 MTX 组的差异具有统计学意义。治疗组的严重不良事件(AE)发生率相似,而包括感染在内的某些治疗后出现的 AE 发生率增加。报告了 3 例死亡,均发生在 MTX 单药治疗组。1 例接受 MTX 单药治疗的患者、1 例接受巴利昔替尼单药治疗的患者和 4 例接受巴利昔替尼联合 MTX 治疗的患者报告了恶性肿瘤,包括非黑色素瘤皮肤癌。