Leiden University Medical Center, Albinusdreef 2, 2333, ZA, Leiden, The Netherlands.
Pôle de Pathologies Rhumatismales Inflammatoires et Systémiques, Institut de Recherche Expérimentale et Clinique, Université Catholique de Louvain and Service de Rhumatologie, Cliniques Universitaires Saint-Luc, Brussels, Belgium.
Clin Rheumatol. 2018 Sep;37(9):2381-2390. doi: 10.1007/s10067-018-4221-0. Epub 2018 Aug 4.
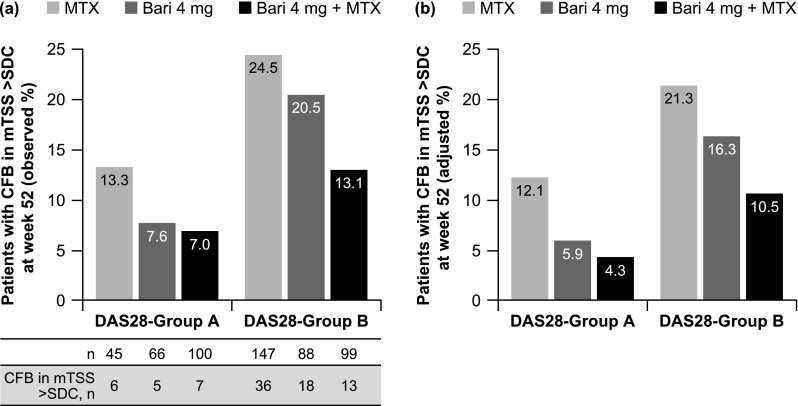
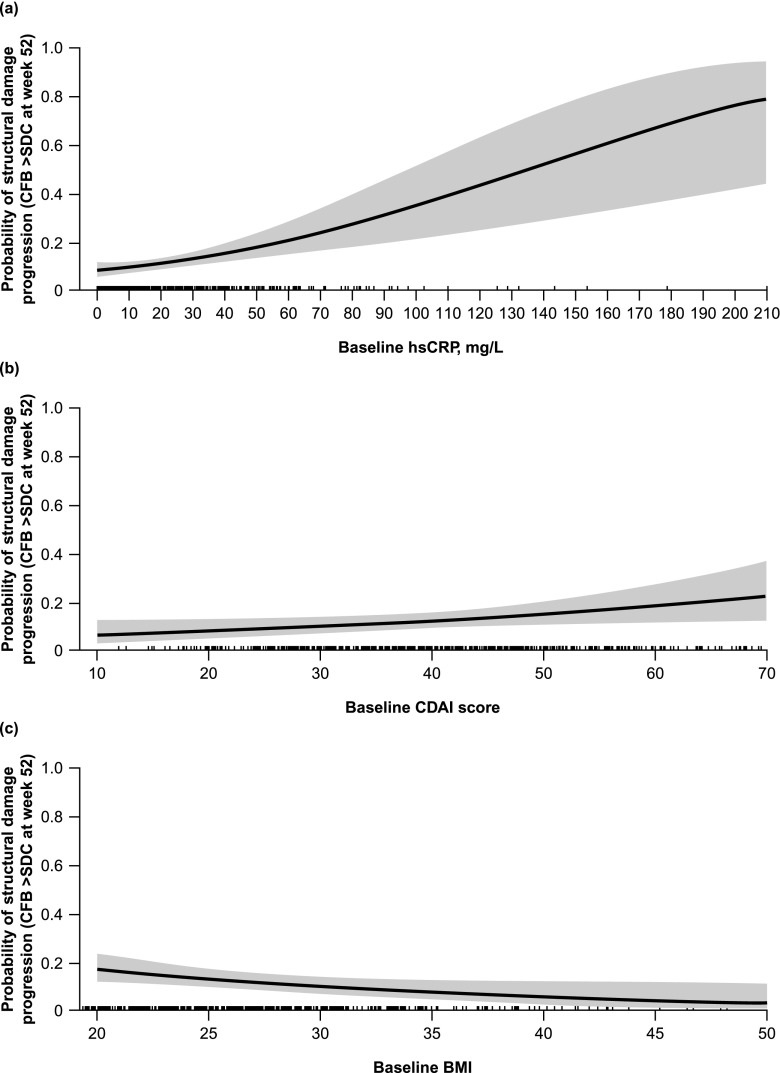
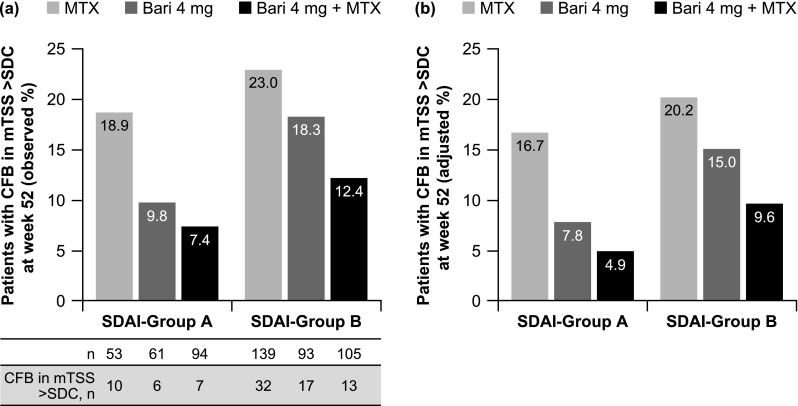
The objective of this study was to evaluate structural damage progression based on clinical response in rheumatoid arthritis patients with no or limited prior disease-modifying anti-rheumatic drug treatment receiving the Janus kinase (JAK)1/JAK2 inhibitor baricitinib 4 mg, methotrexate (MTX), or the combination. Data from the phase 3 RA-BEGIN study were analysed post hoc. Proportions of patients with structural damage progression (change from baseline greater than the smallest detectable change in modified total Sharp score) at week 52 were evaluated based on sustained Disease Activity Score for 28-joint count with serum high-sensitivity C-reactive protein (DAS28-hsCRP) ≤ 3.2 or Simplified Disease Activity Index (SDAI) score ≤ 11; no formal statistical comparisons between treatments were performed to test these proportions. Baseline factors associated with risk of structural damage progression, including Clinical Disease Activity Index (CDAI) score, were identified using multivariate analysis. Patients achieving versus not achieving sustained DAS28-hsCRP ≤ 3.2 or SDAI score ≤ 11 were less likely to experience structural damage progression at week 52. In patients achieving these responses, structural damage progression was less likely with baricitinib monotherapy or plus MTX than with MTX monotherapy. In patients not achieving these sustained clinical thresholds, structural damage progression was less likely with baricitinib plus MTX than with either monotherapy. Independent of treatment, baseline factors significantly associated with increased risk of structural damage progression included higher hsCRP and CDAI score, smoking, female sex, and lower body mass index. In conclusion, patients achieving versus not achieving sustained DAS28-hsCRP ≤ 3.2 or SDAI score ≤ 11 were less likely to show structural damage progression, irrespective of treatment.
本研究的目的是评估在接受 Janus 激酶(JAK)1/JAK2 抑制剂巴瑞替尼 4mg、甲氨蝶呤(MTX)或二者联合治疗、既往无或有限疾病修饰抗风湿药物(DMARD)治疗的类风湿关节炎(RA)患者中,基于临床应答评估结构损伤进展。对 3 期 RA-BEGIN 研究的数据进行了事后分析。根据持续的 28 关节疾病活动度评分(DAS28)与血清高敏 C 反应蛋白(hsCRP)≤3.2 或简化疾病活动指数(SDAI)评分≤11 的缓解,评估第 52 周时发生结构损伤进展(从基线变化大于改良总 Sharp 评分的最小可检测变化)的患者比例;未对治疗组间进行正式的统计学比较以检验这些比例。使用多变量分析确定与结构损伤进展风险相关的基线因素,包括临床疾病活动度指数(CDAI)评分。与未达到持续 DAS28-hsCRP≤3.2 或 SDAI 评分≤11 的患者相比,达到持续缓解的患者在第 52 周时更不可能发生结构损伤进展。在达到这些应答的患者中,与 MTX 单药治疗相比,巴瑞替尼单药或联合 MTX 治疗发生结构损伤进展的可能性更小。在未达到这些持续临床阈值的患者中,与 MTX 单药治疗相比,巴瑞替尼联合 MTX 治疗发生结构损伤进展的可能性更小。无论治疗如何,与结构损伤进展风险显著相关的基线因素包括较高的 hsCRP 和 CDAI 评分、吸烟、女性和较低的体重指数。总之,与未达到持续缓解的患者相比,达到持续 DAS28-hsCRP≤3.2 或 SDAI 评分≤11 的患者发生结构损伤进展的可能性更小,无论治疗如何。