Saccone Gabriele, Berghella Vincenzo
Department of Neuroscience, Reproductive Sciences and Dentistry, School of Medicine, University of Naples Federico II, Naples, Italy.
Division of Maternal-Fetal Medicine, Department of Obstetrics and Gynecology, Sidney Kimmel Medical College of Thomas Jefferson University, Philadelphia, PA 19107, USA
BMJ. 2016 Oct 12;355:i5044. doi: 10.1136/bmj.i5044.
To evaluate the effectiveness of antenatal corticosteroids given at ≥34 weeks' gestation.
Systematic review with meta-analysis.
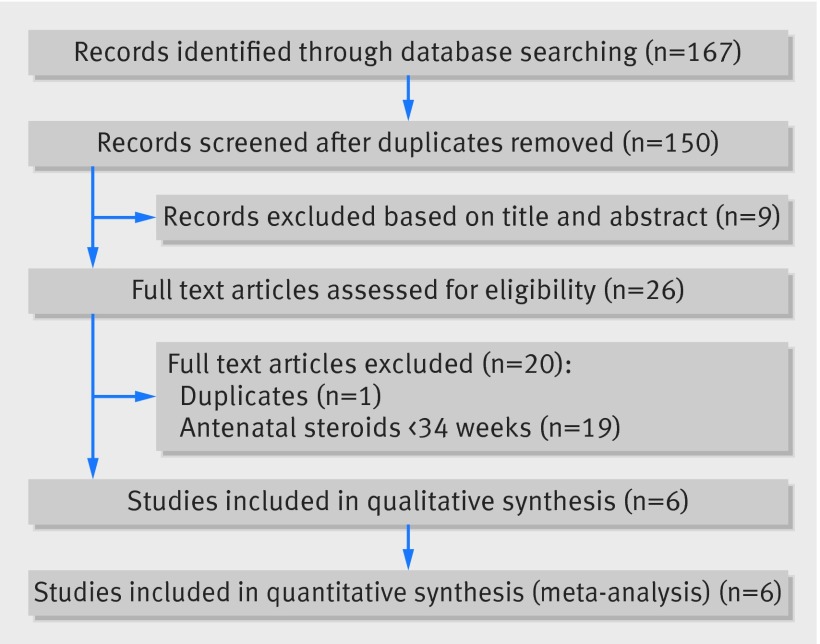
Electronic databases were searched from their inception to February 2016.
Randomized clinical trials comparing antenatal corticosteroids with placebo or no treatment in women with a singleton pregnancy at ≥34 weeks' gestation. Trials on antenatal steroids in women expected to deliver late preterm (34-36 weeks) and trials given before planned cesarean delivery at term (≥37 weeks) were included.
The primary outcome was the incidence of severe respiratory distress syndrome (RDS). The summary measures were reported as relative risks or mean differences with 95% confidence intervals.
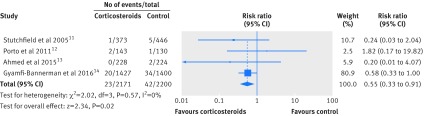
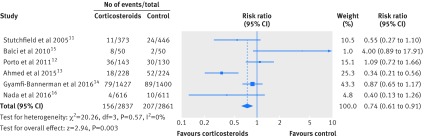
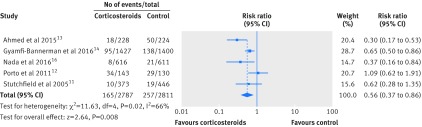
Six trials, including 5698 singleton pregnancies, were analyzed. Three included 3200 women at 34-36 weeks' gestation and at risk of imminent premature delivery at the time of hospital admission. The three other trials included 2498 women undergoing planned cesarean delivery at ≥37 weeks. Overall, infants of mothers who received antenatal corticosteroids at ≥34 weeks had a significantly lower risk of RDS (relative risk 0.74, 95% confidence interval 0.61 to 0.91), mild RDS (0.67, 0.46 to 0.96), moderate RDS (0.39, 0.18 to 0.89), transient tachypnea of the newborn (0.56, 0.37 to 0.86), severe RDS (0.55, 0.33 to 0.91), use of surfactant, and mechanical ventilation, and a significantly lower time receiving oxygen (mean difference -2.06 hours, 95% confidence interval -2.17 to -1.95), lower maximum inspired oxygen concentration (-0.66%, -0.69% to -0.63%), shorter stay on a neonatal intensive care unit (-7.64 days, -7.65 to -7.64), and higher APGAR scores compared with controls. Infants of mothers who received antenatal betamethasone at 34-36 weeks' gestation had a significantly lower incidence of transient tachypnea of the newborn (relative risk 0.72, 95% confidence interval 0.56 to 0.92), severe RDS (0.60, 0.33 to 0.94), and use of surfactant (0.61, 0.38 to 0.99). Infants of mothers undergoing planned cesarean delivery at ≥37 weeks' gestation who received prophylactic antenatal corticosteroids 48 hours before delivery had a significantly lower risk of RDS (0.40, 0.27 to 0.59), mild RDS (0.43, 0.26 to 0.72), moderate RDS (0.40, 0.18 to 0.88), transient tachypnea of the newborn (0.38, 0.25 to 0.57), and mechanical ventilation (0.19, 0.08 to 0.43), and significantly less time receiving oxygen (mean difference -2.06 hours, 95% confidence interval -2.17 to -1.95), lower percentage of maximum inspired oxygen concentration (-0.66%, -0.69% to -0.63%), shorter stay in neonatal intensive care (-7.44 days, -7.44 to -7.43), and a higher APGAR score at one and at five minutes.
Antenatal steroids at ≥34 weeks' gestation reduce neonatal respiratory morbidity. A single course of corticosteroids can be considered for women at risk of imminent late premature delivery 34-36 weeks' gestation, as well as for women undergoing planned cesarean delivery at ≥37 weeks' gestation.
PROSPERO CRD42016035234.
评估妊娠≥34周时给予产前糖皮质激素的有效性。
系统评价与荟萃分析。
检索电子数据库自其创建至2016年2月的数据。
随机临床试验,比较妊娠≥34周的单胎妊娠妇女产前糖皮质激素与安慰剂或不治疗的效果。纳入预期早产(34 - 36周)妇女产前使用类固醇的试验以及足月(≥37周)计划剖宫产术前使用类固醇的试验。
主要结局是严重呼吸窘迫综合征(RDS)的发生率。汇总测量结果以相对风险或平均差值及95%置信区间报告。
分析了6项试验,包括5698例单胎妊娠。其中3项试验纳入了3200例妊娠34 - 36周、入院时面临即将早产风险的妇女。另外3项试验纳入了2498例≥37周行计划剖宫产的妇女。总体而言,妊娠≥34周接受产前糖皮质激素治疗的母亲所生婴儿发生RDS的风险显著降低(相对风险0.74,95%置信区间0.61至0.91),轻度RDS(0.67,0.46至0.96),中度RDS(0.39,0.18至0.89),新生儿短暂性呼吸急促(0.56,0.37至0.86),严重RDS(0.55,0.33至0.91),使用表面活性剂和机械通气的风险也显著降低,吸氧时间显著缩短(平均差值 - 2.06小时,95%置信区间 - 2.17至 - 1.95),最高吸入氧浓度降低(-0.66%,-0.69%至 - 0.63%),新生儿重症监护病房住院时间缩短(-7.64天,-7.65至 - 7.64),与对照组相比,阿氏评分更高。妊娠34 - 36周接受产前倍他米松治疗的母亲所生婴儿发生新生儿短暂性呼吸急促(相对风险0.72,95%置信区间0.56至0.92)、严重RDS(0.60,0.33至0.94)和使用表面活性剂(0.61,0.38至0.99)的发生率显著降低。≥37周行计划剖宫产的母亲在分娩前48小时接受预防性产前糖皮质激素治疗,其婴儿发生RDS(0.40,0.27至0.59)、轻度RDS(0.43,0.26至0.72)、中度RDS(0.40,0.18至0.88)、新生儿短暂性呼吸急促(0.38,0.25至0.57)和机械通气(0.19,0.08至0.43)的风险显著降低,吸氧时间显著缩短(平均差值 - 2.06小时,95%置信区间 - 2.17至 - 1.95),最高吸入氧浓度百分比降低(-0.66%,-0.69%至 - 0.63%),新生儿重症监护病房住院时间缩短(-7.44天,-7.44至 - 7.43),1分钟和5分钟时阿氏评分更高。
妊娠≥34周时使用产前类固醇可降低新生儿呼吸系统发病率。对于妊娠34 - 36周面临即将早产风险的妇女以及≥37周行计划剖宫产的妇女,可考虑给予单疗程糖皮质激素治疗。
PROSPERO CRD42016035234