Kurt Ahmet, Ulusoy Can Ozan, Kurt Dilara Sarikaya, Özkan Sadullah, Dereli Murat Levent, Kından Aykut, Çelik Özge Yücel, Uzlu Safiye Elif, Çelen Şevki
Department of Obstetrics and Gynecology, Ankara Etlik City Hospital, Ankara, Turkey.
Department of Perinatology, Etlik City Hospital, Ankara, Turkey.
BMC Pediatr. 2025 Aug 4;25(1):595. doi: 10.1186/s12887-025-05925-w.
This study aimed to evaluate the impact of antenatal corticosteroid therapy (ACT) on neonatal respiratory outcomes in late preterm births, focusing on the interaction between gestational age, mode of delivery, and ACT administration.
A retrospective case-control study was conducted on 452 singleton late preterm pregnancies (34 + 0 to 36 + 6 weeks) between 2014 and 2021. Among these, 197 patients received ACT, while 255 did not. Maternal and neonatal characteristics were collected, and logistic regression analyses were performed to identify predictors of neonatal respiratory complications.
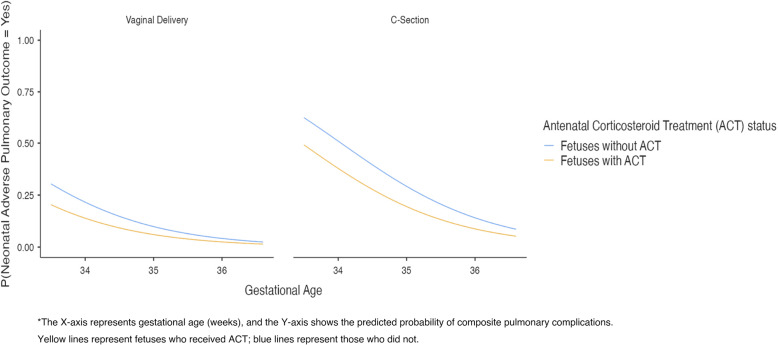
ACT was associated with a 42% reduction in the odds of neonatal pulmonary complications (adjusted OR: 0.586; 95% CI: 0.347–0.988; = 0.045). Gestational age was a significant protective factor, with each additional week reducing the risk of adverse pulmonary outcomes by 60% (adjusted OR: 0.397; 95% CI: 0.281–0.561; < 0.001). Cesarean delivery was associated with a nearly fourfold increase in pulmonary complications compared to vaginal delivery (adjusted OR: 3.775; 95% CI: 1.859–7.666; < 0.001). ACT showed the most significant protective effect in earlier gestational weeks and among cesarean deliveries.
ACT was associated with reduced neonatal pulmonary complications in late preterm pregnancies, particularly among subgroups with earlier gestational age or cesarean delivery, as supported by multivariate and interaction analyses. These findings underscore the importance of individualized antenatal and perinatal management strategies to optimize neonatal outcomes.
本研究旨在评估产前皮质类固醇疗法(ACT)对晚期早产新生儿呼吸结局的影响,重点关注胎龄、分娩方式与ACT给药之间的相互作用。
对2014年至2021年间452例单胎晚期早产妊娠(34⁺⁰至36⁺⁶周)进行回顾性病例对照研究。其中,197例患者接受了ACT,255例未接受。收集产妇和新生儿特征,并进行逻辑回归分析以确定新生儿呼吸并发症的预测因素。
ACT与新生儿肺部并发症几率降低42%相关(调整后OR:0.586;95%CI:0.347 - 0.988;P = 0.045)。胎龄是一个显著的保护因素,每增加一周,不良肺部结局风险降低60%(调整后OR:0.397;95%CI:0.281 - 0.561;P < 0.001)。与阴道分娩相比,剖宫产与肺部并发症增加近四倍相关(调整后OR:3.775;95%CI:1.859 - 7.666;P < 0.001)。ACT在较早孕周和剖宫产中显示出最显著的保护作用。
多因素和相互作用分析支持,ACT与晚期早产妊娠新生儿肺部并发症减少相关,特别是在胎龄较早或剖宫产的亚组中。这些发现强调了个体化产前和围产期管理策略对优化新生儿结局的重要性。