Xeuatvongsa Anonh, Datta Siddhartha Sankar, Moturi Edna, Wannemuehler Kathleen, Philakong Phanmanisone, Vongxay Viengnakhone, Vilayvone Vansy, Patel Minal K
National Immunization Program, Mother and Child Health Center, Lao People's Democratic Republic Ministry of Health, Simuang Road, Vientiane, Lao Democratic People's Republic.
WHO Representative Office in Laos, 125 Saphanthong Road, Unit 5, Ban Saphanthongtai, Sisattanak District, Vientiane, Lao Democratic People's Republic.
Vaccine. 2016 Nov 11;34(47):5777-5784. doi: 10.1016/j.vaccine.2016.09.056. Epub 2016 Oct 11.
Hepatitis B vaccine birth dose (HepB-BD) was introduced in Lao People's Democratic Republic to prevent perinatal hepatitis B virus transmission in 2008; high coverage is challenging since only 38% of births occur in a health facility. Healthcare workers report being unaware of home births and thus unable to conduct timely postnatal care (PNC) home visits. A quasi-experimental pilot study was conducted wherein mobile phones and phone credits were provided to village health volunteers (VHV) and healthcare workers (HCWs) to assess whether this could improve HepB-BD administration, as well as birth notification and increase home visits.
From April to September 2014, VHVs and HCWs in four selected intervention districts were trained, supervised, received outreach per diem for conducting home visits, and received mobile phones and phone credits. In three comparison districts, VHVs and HCWs were trained, supervised, and received outreach per diem for conducting home visits. A post-study survey compared HepB-BD coverage among children born during the study and children born one year before. HCWs and VHVs were interviewed about the study.
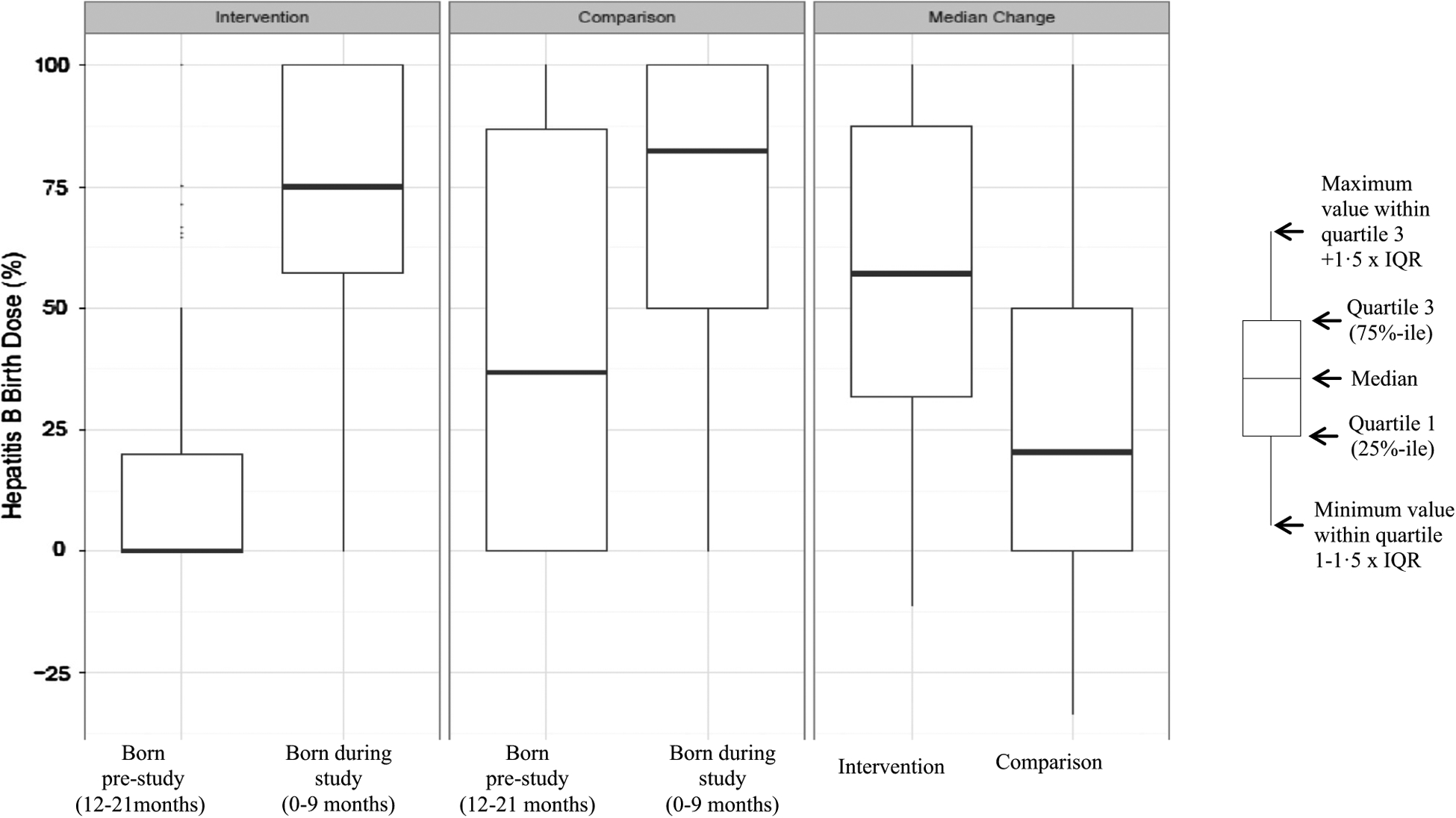
Among intervention districts, 463 study children and 406 pre-study children were enrolled in the survey; in comparison districts, 347 study children and 309 pre-study children were enrolled. In both arms, there was a significant improvement in the proportion of children reportedly receiving a PNC home visit (intervention p<0.0001, comparison p=0.04). The median difference in village level HepB-BD coverage (study cohort minus pre-study cohort), was 57% (interquartile range [IQR] 32-88%, p<0.0001) in intervention districts, compared with 20% (IQR 0-50%, p<0.0001) in comparison districts. The improvement in the intervention districts was greater than in the comparison districts (p=0.0009).
Our findings suggest that the provision of phones and phone credits might be one important factor for increasing coverage. However, reasons for improvement in both arms are multifactorial and discussed.
2008年,老挝人民民主共和国引入了乙肝疫苗首剂接种(HepB-BD)以预防围产期乙肝病毒传播;由于只有38%的分娩在医疗机构进行,实现高覆盖率具有挑战性。医护人员报告称不了解家庭分娩情况,因此无法及时进行产后护理(PNC)家访。开展了一项准实验性试点研究,向乡村卫生志愿者(VHV)和医护人员(HCW)提供手机和电话费用,以评估这是否能改善乙肝疫苗首剂接种情况以及出生报告,并增加家访次数。
2014年4月至9月,对四个选定干预区的乡村卫生志愿者和医护人员进行培训、监督,为其进行家访提供外联每日津贴,并提供手机和电话费用。在三个对照区,对乡村卫生志愿者和医护人员进行培训、监督,并为其进行家访提供外联每日津贴。一项研究后调查比较了研究期间出生儿童和一年前出生儿童的乙肝疫苗首剂接种覆盖率。对医护人员和乡村卫生志愿者进行了关于该研究的访谈。
在干预区,463名研究儿童和406名研究前儿童参与了调查;在对照区,347名研究儿童和309名研究前儿童参与了调查。在两组中,据报告接受产后护理家访的儿童比例均有显著提高(干预组p<0.0001,对照组p=0.04)。干预区村级乙肝疫苗首剂接种覆盖率的中位数差异(研究队列减去研究前队列)为57%(四分位间距[IQR]32 - 88%,p<0.0001),而对照区为20%(IQR 0 - 50%,p<0.0001)。干预区的改善幅度大于对照区(p=0.0009)。
我们的研究结果表明,提供手机和电话费用可能是提高覆盖率的一个重要因素。然而,两组改善的原因是多因素的,并进行了讨论。