Walter Christian, Al-Nawas Bilal, Wolff Tim, Schiegnitz Eik, Grötz Knut A
Department of Oral and Maxillofacial Surgery - Plastic Surgery of the Johannes Gutenberg-University Mainz, Augustusplatz 2, 55131, Mainz, Germany.
Department of Oral and Maxillofacial Surgery of the Dr. Horst Schmidt Clinic, Ludwig-Erhard-Str. 100, 65199, Wiesbaden, Germany.
Int J Implant Dent. 2016 Dec;2(1):9. doi: 10.1186/s40729-016-0041-7. Epub 2016 Apr 4.
Bisphosphonate-associated osteonecrosis of the jaws (BP-ONJ) is triggered by inflammatory processes. Typical trigger factors are periodontal disease, denture pressure sores, and surgical interventions such as tooth extractions. Unfortunately there is only little data on how to proceed with implant therapy in patients with bisphosphonate treatment. This topic is not addressed in the German guidelines on medication-associated osteonecrosis. Therefore a systematic literature review was performed.
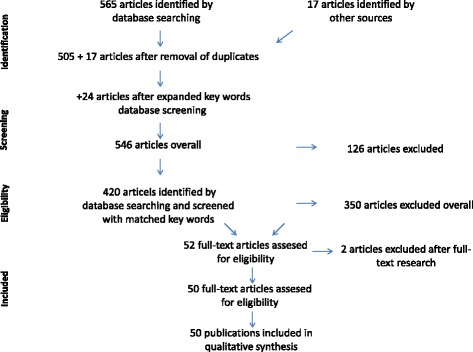
The PICO design was used: (Patients) For which subclientel of patients with antiresorptive therapy (intervention) do dental implants have a benefit (control) compared to forgoing dental implants (outcome) in regards to oral rehabilitation and quality of life without having a substantial risk of BP-ONJ development? A PubMed search was performed including all studies dealing with this topic. Case reports and studies with less than 5 cases were excluded.
There is only very little data available, mostly retrospective case series. 50 articles were analyzed in detail. BP-ONJ can be triggered by dental implants and by dentures in patients with benign and malignant primary diseases. In most studies, analyzing osteoporosis patients only, no cases of BP-ONJ were observed in patients with implant therapy in the time span observed. There are no studies about implant therapy in patients with malignant diseases. Many case series analyzing the trigger factors for BP-ONJ describe dentures as one of the main causes. Perioperative antimicrobial prophylaxis has a benefit in the prevention of BP-ONJ development.
Successful implant therapy is possible in patients receiving antiresorptive therapy. The possibility of osteonecrosis development needs to be explained to the patient. An individual risk assessment is essential, taking the primary disease with the medication and further wound-healing-compromising diseases and medications into account. If possible, bone augmentations should be avoided, and a perioperative antimicrobiological prophylaxis is strongly recommended in these patients.
双膦酸盐相关颌骨骨坏死(BP-ONJ)由炎症过程引发。典型的触发因素包括牙周病、义齿压迫性溃疡以及诸如拔牙等外科手术干预。遗憾的是,关于双膦酸盐治疗患者如何进行种植治疗的数据极少。德国关于药物相关性骨坏死的指南未涉及该主题。因此,进行了一项系统的文献综述。
采用PICO设计:(患者)对于接受抗吸收治疗的哪类亚组患者(干预措施),与不进行牙种植体植入(对照措施)相比,牙种植体在口腔修复和生活质量方面有获益(结局),且发生BP-ONJ的风险不大?在PubMed上进行了检索,纳入了所有涉及该主题的研究。排除了病例报告和病例数少于5例的研究。
仅有极少的数据,大多为回顾性病例系列。详细分析了50篇文章。BP-ONJ可由牙种植体以及患有良性和恶性原发性疾病患者的义齿引发。在大多数仅分析骨质疏松症患者的研究中,在所观察的时间段内,接受种植治疗的患者未观察到BP-ONJ病例。尚无关于恶性疾病患者种植治疗的研究。许多分析BP-ONJ触发因素的病例系列将义齿描述为主要原因之一。围手术期抗菌预防对预防BP-ONJ的发生有益。
接受抗吸收治疗的患者有可能成功进行种植治疗。需要向患者解释发生骨坏死的可能性。进行个体风险评估至关重要,要考虑原发性疾病、所用药物以及其他会损害伤口愈合的疾病和药物。如果可能,应避免骨增量,强烈建议对这些患者进行围手术期抗菌预防。