Okura Masaya, Yanamoto Souichi, Umeda Masahiro, Otsuru Mitsunobu, Ota Yoshihide, Kurita Hiroshi, Kamata Takahiro, Kirita Tadaaki, Yamakawa Nobuhiro, Yamashita Tetsuro, Ueda Michihiro, Komori Takahide, Hasegawa Takumi, Aikawa Tomonao
The First Department of Oral and Maxillofacial Surgery, Graduate School of Dentistry, Osaka University, Osaka, Japan.
Department of Clinical Oral Oncology, Nagasaki University Graduate School of Biomedical Sciences, Nagasaki, Japan.
Cancer Med. 2016 Dec;5(12):3378-3385. doi: 10.1002/cam4.899. Epub 2016 Oct 19.
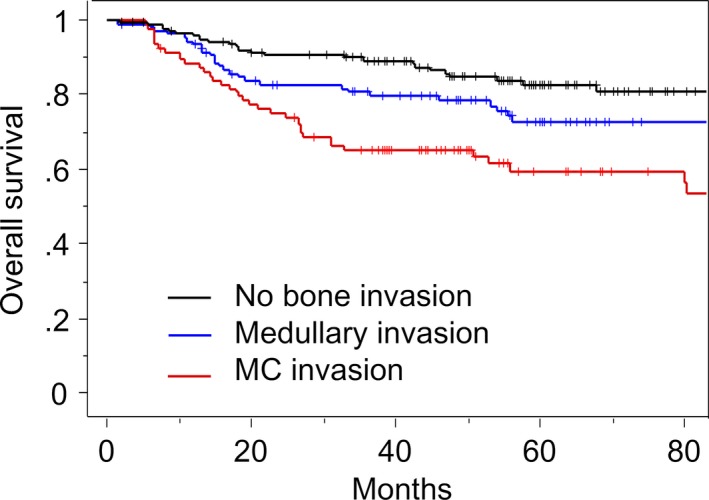
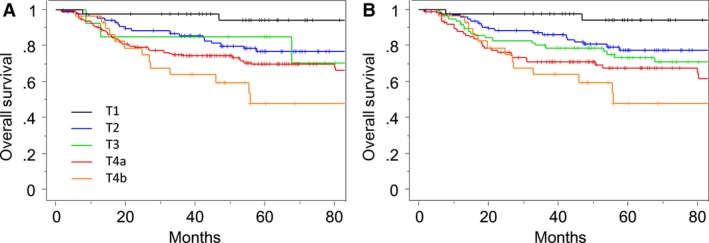
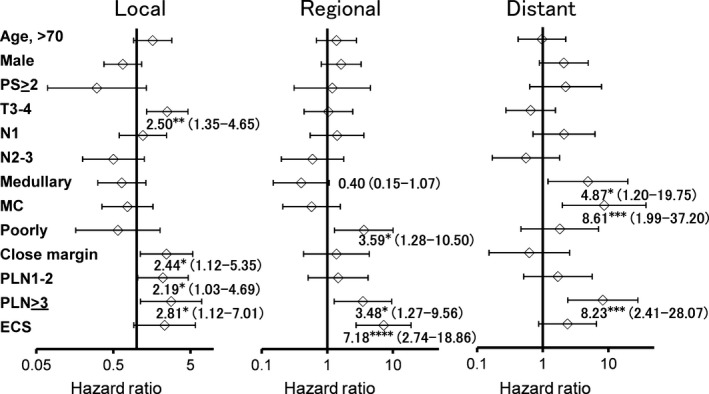
A multi-institutional study was undertaken to determine whether mandibular canal (MC) invasion and mandibular medullary bone invasion are independent factors in lower gingival squamous cell carcinoma (SCC). A total of 345 patients with lower gingival SCC were retrospectively reviewed. Mandibular bone invasion was categorized into three types; no bone invasion; invasion through cortical bone (medullary); and MC invasion. The overall survival rate and factors affecting local, regional, and distant failures were assessed by Cox proportional hazards regression analysis and Kaplan-Meier estimates. Bone invasion was present in 201 (58%) patients, of whom 107 (31%) had medullary invasion and 94 (27%) had MC invasion. Using the International Union Against Cancer (UICC) staging system and American Joint Committee on Cancer (AJCC) system, 171 (50%) patients were classified as T4a. When the bone invasion criteria were excluded from the UICC/AJCC system definition, 152 T4a tumors were downstaged and reclassified to T1 in 12 (3%), to T2 in 98 (28%), and to T3 in 42 (12%). In Cox multivariate analysis, MC invasion was an independent predictor of overall survival but medullary bone invasion was not. Medullary bone invasion was an independent variable for distant control. The current T staging system has restricted prognostic utility. The authors recommend a modified T staging system, whereby tumors with MC invasion instead of medullary bone invasion are classified as T4a, and tumors are first classified as T1 to T3 based on size and then upstaged by one T classification in the presence of medullary invasion.
一项多机构研究旨在确定下颌管(MC)侵犯和下颌骨髓骨侵犯是否为下牙龈鳞状细胞癌(SCC)的独立影响因素。对345例下牙龈SCC患者进行了回顾性研究。下颌骨侵犯分为三种类型:无骨侵犯;穿破皮质骨(骨髓)侵犯;以及MC侵犯。通过Cox比例风险回归分析和Kaplan-Meier估计评估总生存率以及影响局部、区域和远处复发的因素。201例(58%)患者存在骨侵犯,其中107例(31%)有骨髓侵犯,94例(27%)有MC侵犯。根据国际抗癌联盟(UICC)分期系统和美国癌症联合委员会(AJCC)系统,171例(50%)患者被归类为T4a。当从UICC/AJCC系统定义中排除骨侵犯标准时,152例T4a肿瘤分期降低,其中12例(3%)重新分类为T1,98例(28%)重新分类为T2,42例(12%)重新分类为T3。在Cox多因素分析中,MC侵犯是总生存率的独立预测因素,而骨髓骨侵犯不是。骨髓骨侵犯是远处控制的独立变量。当前的T分期系统预后效用有限。作者建议采用改良的T分期系统,即有MC侵犯而非骨髓骨侵犯的肿瘤分类为T4a,肿瘤首先根据大小分类为T1至T3,然后在存在骨髓侵犯时T分期上调一级。