Hegarty Joanne Elizabeth, Harding Jane Elizabeth, Gamble Gregory David, Crowther Caroline Anne, Edlin Richard, Alsweiler Jane Marie
Liggins Institute, University of Auckland, Auckland, New Zealand.
Newborn Services, National Women's Health, Auckland, New Zealand.
PLoS Med. 2016 Oct 25;13(10):e1002155. doi: 10.1371/journal.pmed.1002155. eCollection 2016 Oct.
Neonatal hypoglycaemia is common, affecting up to 15% of newborns, and can cause brain damage. Currently, there are no strategies, beyond early feeding, to prevent neonatal hypoglycaemia. Our aim was to determine a dose of 40% oral dextrose gel that will prevent neonatal hypoglycaemia in newborn babies at risk.
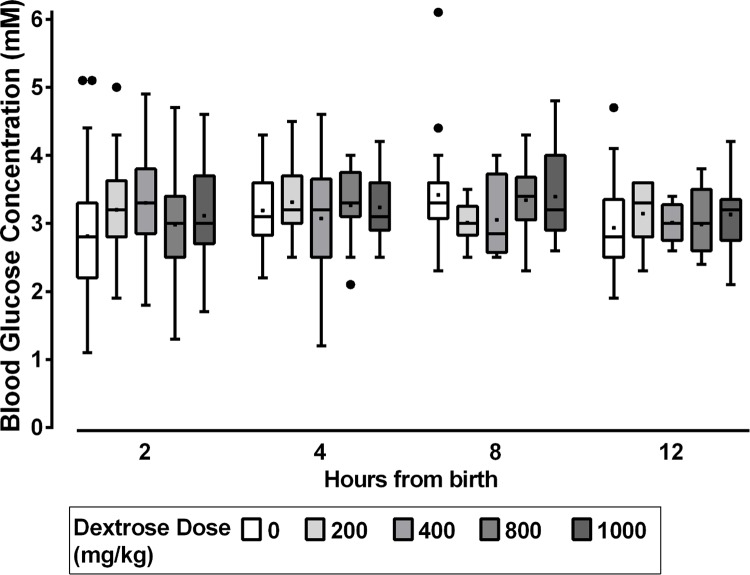
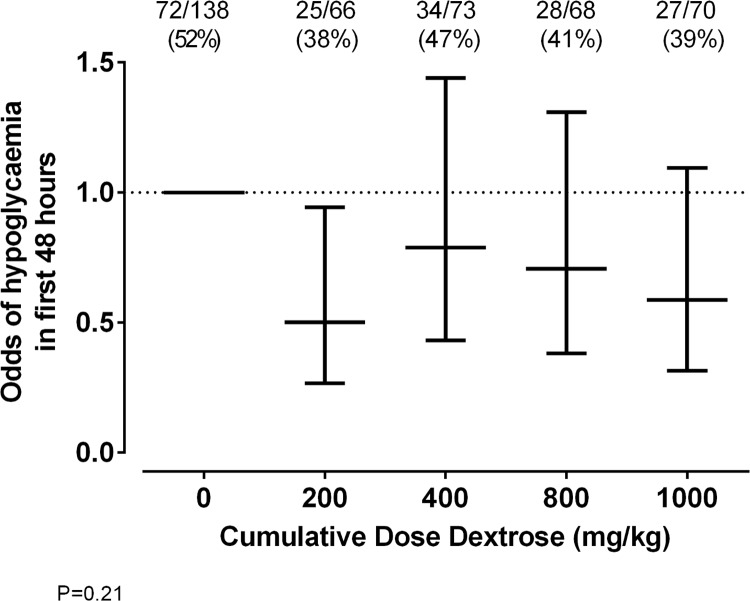
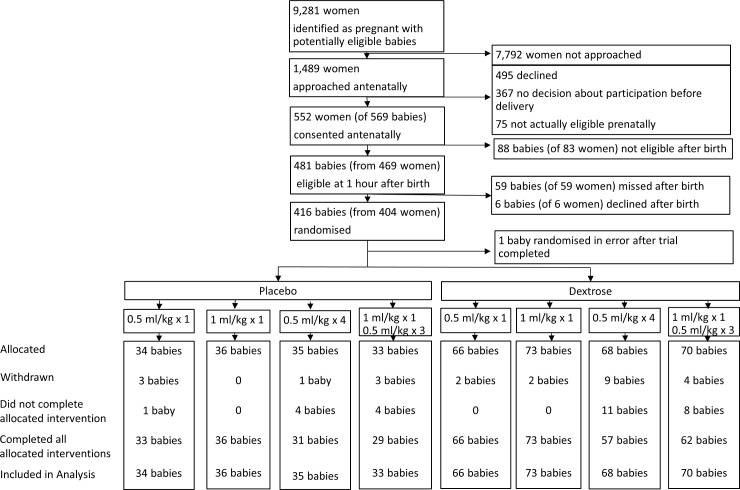
We conducted a randomised, double-blind, placebo-controlled dose-finding trial of buccal dextrose gel to prevent neonatal hypoglycaemia at two hospitals in New Zealand. Babies at risk of hypoglycaemia (infant of a mother with diabetes, late preterm delivery, small or large birthweight, or other risk factors) but without indication for admission to a neonatal intensive care unit (NICU) were randomly allocated either to one of four treatment groups: 40% dextrose at one of two doses (0.5 ml/kg = 200 mg/kg, or 1 ml/kg = 400 mg/kg), either once at 1 h of age or followed by three additional doses of dextrose (0.5 ml/kg before feeds in the first 12 h); or to one of four corresponding placebo groups. Treatments were administered by massaging gel into the buccal mucosa. The primary outcome was hypoglycaemia (<2.6 mM) in the first 48 h. Secondary outcomes included admission to a NICU, admission for hypoglycaemia, and breastfeeding at discharge and at 6 wk. Prespecified potential dose limitations were tolerance of gel, time taken to administer, messiness, and acceptability to parents. From August 2013 to November 2014, 416 babies were randomised. Compared to babies randomised to placebo, the risk of hypoglycaemia was lowest in babies randomised to a single dose of 200 mg/kg dextrose gel (relative risk [RR] 0.68; 95% confidence interval [CI] 0.47-0.99, p = 0.04) but was not significantly different between dose groups (p = 0.21). Compared to multiple doses, single doses of gel were better tolerated, quicker to administer, and less messy, but these limitations were not different between dextrose and placebo gel groups. Babies who received any dose of dextrose gel were less likely to develop hypoglycaemia than those who received placebo (RR 0.79; 95% CI 0.64-0.98, p = 0.03; number needed to treat = 10, 95% CI 5-115). Rates of NICU admission were similar (RR 0.64; 95% CI 0.33-1.25, p = 0.19), but admission for hypoglycaemia was less common in babies randomised to dextrose gel (RR 0.46; 95% CI 0.21-1.01, p = 0.05). Rates of breastfeeding were similar in both groups. Adverse effects were uncommon and not different between groups. A limitation of this study was that most of the babies in the trial were infants of mothers with diabetes (73%), which may reduce the applicability of the results to babies from other risk groups.
The incidence of neonatal hypoglycaemia can be reduced with a single dose of buccal 40% dextrose gel 200 mg/kg. A large randomised trial (Hypoglycaemia Prevention with Oral Dextrose [hPOD]) is under way to determine the effects on NICU admission and later outcomes.
Australian New Zealand Clinical Trials Registry ACTRN12613000322730.
新生儿低血糖很常见,影响高达15%的新生儿,并可能导致脑损伤。目前,除了早期喂养外,没有预防新生儿低血糖的策略。我们的目的是确定一种40%口服葡萄糖凝胶的剂量,该剂量将预防有风险的新生儿发生低血糖。
我们在新西兰的两家医院进行了一项随机、双盲、安慰剂对照的剂量探索试验,以研究颊部葡萄糖凝胶预防新生儿低血糖的效果。有低血糖风险的婴儿(母亲患有糖尿病、晚期早产、出生体重过小或过大或有其他风险因素)但无入住新生儿重症监护病房(NICU)指征的,被随机分配到四个治疗组之一:两种剂量之一的40%葡萄糖(0.5 ml/kg = 200 mg/kg,或1 ml/kg = 400 mg/kg),在1小时龄时给药一次,或随后再额外给药三次葡萄糖(在最初12小时内每次喂奶前0.5 ml/kg);或四个相应的安慰剂组之一。通过将凝胶按摩到颊黏膜来给药。主要结局是出生后48小时内的低血糖(<2.6 mM)。次要结局包括入住NICU、因低血糖入院以及出院时和6周时的母乳喂养情况。预先设定的潜在剂量限制因素包括凝胶的耐受性、给药所需时间、脏乱程度以及父母的接受度。从2013年8月至2014年11月,416名婴儿被随机分组。与随机分配到安慰剂组的婴儿相比,随机分配到单剂量200 mg/kg葡萄糖凝胶的婴儿发生低血糖的风险最低(相对风险[RR] 0.68;95%置信区间[CI] 0.47 - 0.99,p = 0.04),但各剂量组之间无显著差异(p = 0.21)。与多次给药相比,单剂量凝胶的耐受性更好、给药更快且更不脏乱,但葡萄糖凝胶组和安慰剂凝胶组在这些限制方面并无差异。接受任何剂量葡萄糖凝胶的婴儿发生低血糖的可能性低于接受安慰剂的婴儿(RR 0.79;95% CI 0.64 - 0.98,p = 0.03;需治疗人数 = 10,95% CI 5 - 115)。NICU入住率相似(RR 0.64;95% CI 0.33 - 1.25,p = 0.19),但随机分配到葡萄糖凝胶组的婴儿因低血糖入院的情况较少见(RR 0.46;95% CI 0.21 - 1.01,p = 0.05)。两组的母乳喂养率相似。不良反应不常见,且组间无差异。本研究的一个局限性是试验中的大多数婴儿是母亲患有糖尿病的婴儿(73%),这可能会降低研究结果对其他风险组婴儿的适用性。
单剂量颊部200 mg/kg的40%葡萄糖凝胶可降低新生儿低血糖的发生率。一项大型随机试验(口服葡萄糖预防低血糖[hPOD])正在进行,以确定其对入住NICU及后续结局的影响。
澳大利亚新西兰临床试验注册中心ACTRN12613000322730。