Park Keun Young, Kim Byung Moon, Kim Dong Joon
Department of Neurosurgery, Severance Hospital, Yonsei University College of Medicine, Seoul 03722, Korea.
Department of Radiology, Severance Hospital, Yonsei University College of Medicine, Seoul 03722, Korea.
Korean J Radiol. 2016 Nov-Dec;17(6):931-939. doi: 10.3348/kjr.2016.17.6.931. Epub 2016 Oct 31.
Few studies have investigated treatment strategies for brain tumor with a coexisting unruptured intracranial aneurysm (cUIA). The purpose of this study was to evaluate the safety and efficacy of preoperative coiling for cUIA, and subsequent brain tumor surgery.
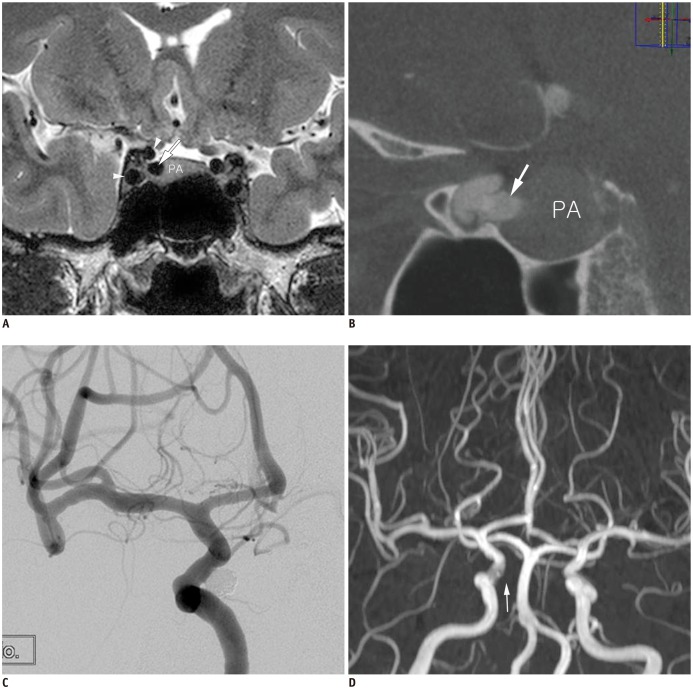
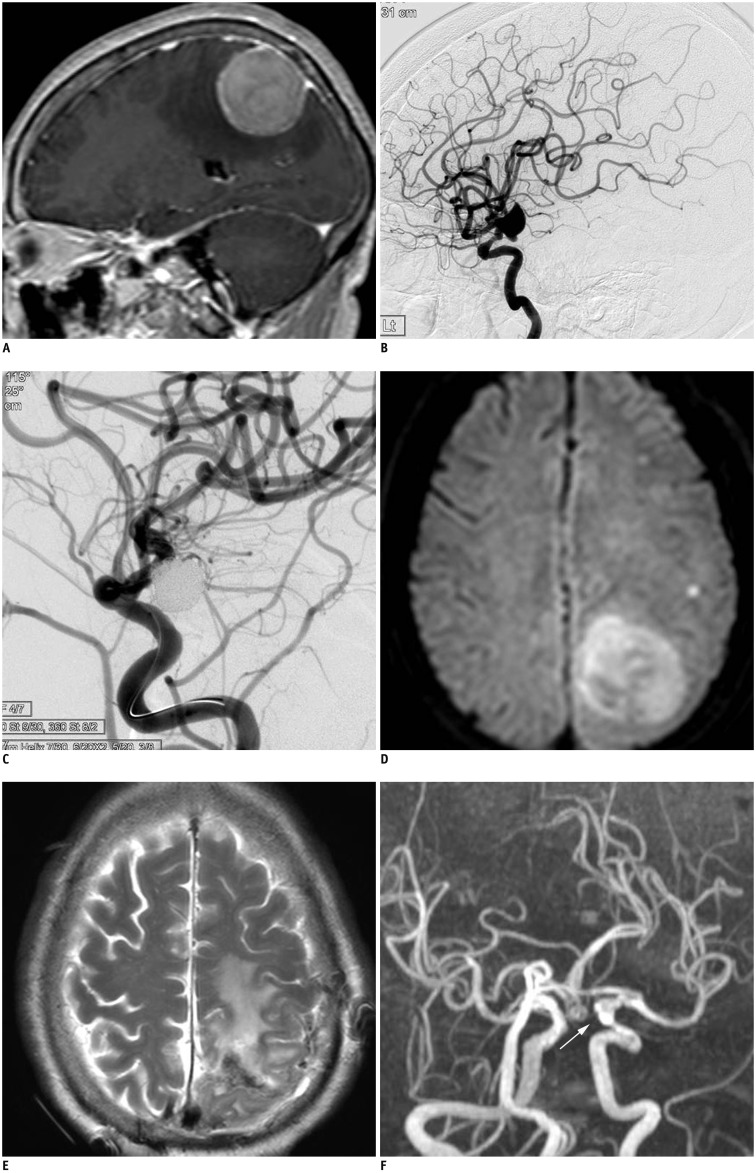
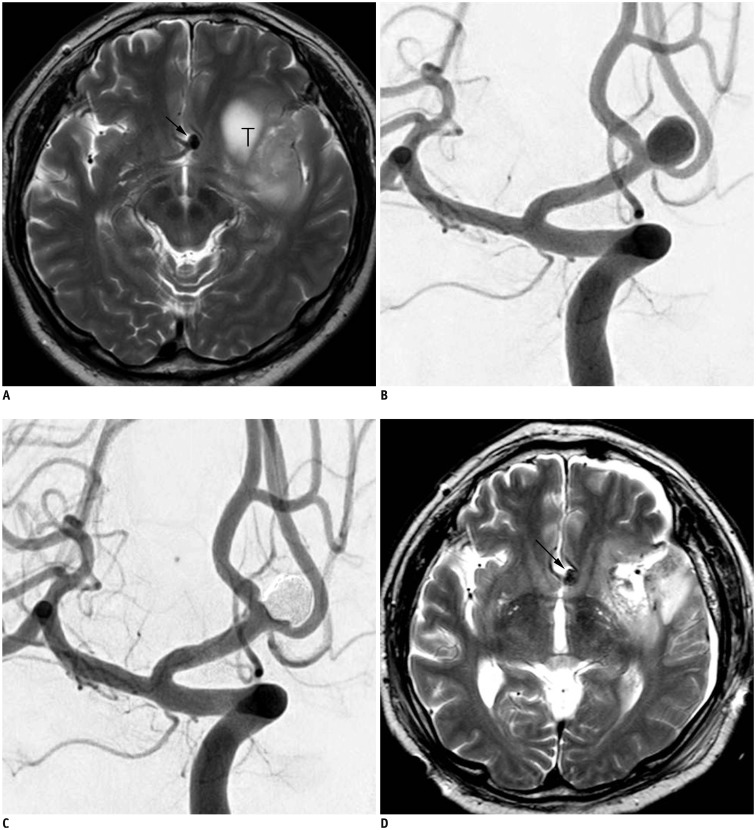
A total of 19 patients (mean age, 55.2 years; M:F = 4:15) underwent preoperative coiling for 23 cUIAs and subsequent brain tumor surgery. Primary brain tumors were meningiomas (n = 7, 36.8%), pituitary adenomas (n = 7, 36.8%), gliomas (n = 3, 15.8%), vestibular schwannoma (n = 1, 5.3%), and Rathke's cleft cyst (n = 1, 5.3%). cUIAs were located at the distal internal carotid artery (n = 9, 39.1%), anterior cerebral artery (n = 8, 34.8%), middle cerebral artery (n = 4, 17.4%), basilar artery top (n = 1, 4.3%), and posterior cerebral artery, P1 segment (n = 1, 4.3%). The outcomes of preoperative coiling of cUIA and subsequent brain tumor surgery were retrospectively evaluated.
Single-microcatheter technique was used in 13 cases (56.5%), balloon-assisted in 4 cases (17.4%), double-microcatheter in 4 cases (17.4%), and stent-assisted in 2 cases (8.7%). Complete cUIA occlusion was achieved in 18 cases (78.3%), while residual neck occurred in 5 cases (21.7%). The only coiling-related complication was 1 transient ischemic attack (5.3%). Neurological deterioration did not occur in any patient during the period between coiling and tumor surgery. At the latest clinical follow-up (mean, 29 months; range, 2-120 months), 15 patients (78.9%) had favorable outcomes (modified Rankin Scale, 0-2), while 4 patients (21.1%) had unfavorable outcomes due to consequences of brain tumor surgery.
Preoperative coiling and subsequent tumor surgery was safe and effective, making it a reasonable treatment option for patients with brain tumor and cUIA.
很少有研究探讨合并未破裂颅内动脉瘤(cUIA)的脑肿瘤的治疗策略。本研究的目的是评估cUIA术前栓塞及随后脑肿瘤手术的安全性和有效性。
共有19例患者(平均年龄55.2岁;男∶女 = 4∶15)接受了23个cUIA的术前栓塞及随后的脑肿瘤手术。原发性脑肿瘤包括脑膜瘤(n = 7,36.8%)、垂体腺瘤(n = 7,36.8%)、胶质瘤(n = 3,15.8%)、前庭神经鞘瘤(n = 1,5.3%)和拉克氏囊肿(n = 1,5.3%)。cUIA位于颈内动脉远端(n = 9,39.1%)、大脑前动脉(n = 8,34.8%)、大脑中动脉(n = 4,17.4%)、基底动脉顶端(n = 1,4.3%)和大脑后动脉P1段(n = 1,4.3%)。对cUIA术前栓塞及随后脑肿瘤手术的结果进行回顾性评估。
13例(56.5%)采用单微导管技术,4例(17.4%)采用球囊辅助,4例(17.4%)采用双微导管,2例(8.7%)采用支架辅助。18例(78.3%)实现了cUIA完全闭塞,5例(21.7%)有残余瘤颈。唯一与栓塞相关的并发症是1例短暂性脑缺血发作(5.3%)。在栓塞与肿瘤手术期间,没有患者发生神经功能恶化。在最近的临床随访中(平均29个月;范围2 - 120个月),15例患者(78.9%)预后良好(改良Rankin量表评分0 - 2分),4例患者(21.1%)因脑肿瘤手术的后果预后不良。
术前栓塞及随后的肿瘤手术安全有效,是合并cUIA的脑肿瘤患者的合理治疗选择。