Vallon Volker, Thomson Scott C
Division of Nephrology and Hypertension, Department of Medicine, University of California San Diego, La Jolla, CA, 92093, USA.
Department of Pharmacology, University of California San Diego, La Jolla, CA, 92093, USA.
Diabetologia. 2017 Feb;60(2):215-225. doi: 10.1007/s00125-016-4157-3. Epub 2016 Nov 22.
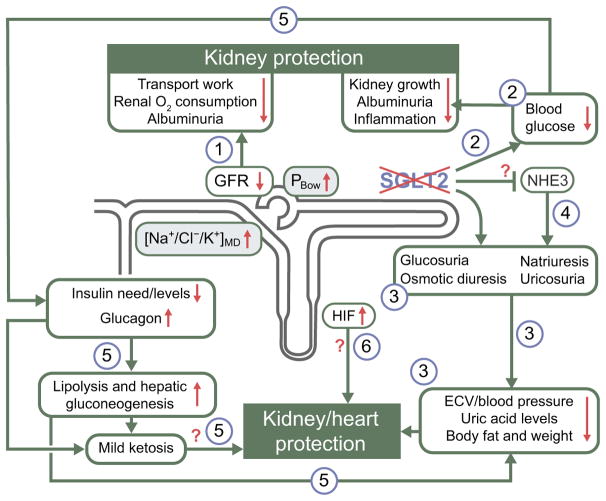
Healthy kidneys filter ∼160 g/day of glucose (∼30% of daily energy intake) under euglycaemic conditions. To prevent valuable energy from being lost in the urine, the proximal tubule avidly reabsorbs filtered glucose up to a limit of ∼450 g/day. When blood glucose levels increase to the point that the filtered load exceeds this limit, the surplus is excreted in the urine. Thus, the kidney provides a safety valve that can prevent extreme hyperglycaemia as long as glomerular filtration is maintained. Most of the capacity for renal glucose reabsorption is provided by sodium glucose cotransporter (SGLT) 2 in the early proximal tubule. In the absence or with inhibition of SGLT2, the renal reabsorptive capacity for glucose declines to ∼80 g/day (the residual capacity of SGLT1), i.e. the safety valve opens at a lower threshold, which makes it relevant to glucose homeostasis from day-to-day. Several SGLT2 inhibitors are now approved glucose lowering agents for individuals with type 2 diabetes and preserved kidney function. By inducing glucosuria, these drugs improve glycaemic control in all stages of type 2 diabetes, while their risk of causing hypoglycaemia is low because they naturally stop working when the filtered glucose load falls below ∼80 g/day and they do not otherwise interfere with metabolic counterregulation. Through glucosuria, SGLT2 inhibitors reduce body weight and body fat, and shift substrate utilisation from carbohydrates to lipids and, possibly, ketone bodies. Because SGLT2 reabsorbs sodium along with glucose, SGLT2 blockers are natriuretic and antihypertensive. Also, because they work in the proximal tubule, SGLT2 inhibitors increase delivery of fluid and electrolytes to the macula densa, thereby activating tubuloglomerular feedback and increasing tubular back pressure. This mitigates glomerular hyperfiltration, reduces the kidney's demand for oxygen and lessens albuminuria. For reasons that are less well understood, SGLT2 inhibitors are also uricosuric. These pleiotropic effects of SGLT2 inhibitors are likely to have contributed to the results of the EMPA-REG OUTCOME trial in which the SGLT2 inhibitor, empagliflozin, slowed the progression of chronic kidney disease and reduced major adverse cardiovascular events in high-risk individuals with type 2 diabetes. This review discusses the role of SGLT2 in the physiology and pathophysiology of renal glucose reabsorption and outlines the unexpected logic of inhibiting SGLT2 in the diabetic kidney.
在血糖正常的情况下,健康的肾脏每天过滤约160克葡萄糖(约占每日能量摄入的30%)。为防止宝贵的能量随尿液流失,近端小管会积极重吸收过滤后的葡萄糖,直至达到约450克/天的上限。当血糖水平升高到滤过负荷超过此极限时,多余的葡萄糖就会随尿液排出。因此,只要肾小球滤过功能得以维持,肾脏就能起到安全阀的作用,防止出现极度高血糖。肾脏对葡萄糖的重吸收能力主要由近端小管起始段的钠葡萄糖协同转运蛋白(SGLT)2提供。在缺乏SGLT2或其受到抑制时,肾脏对葡萄糖的重吸收能力会降至约80克/天(SGLT1的残余能力),也就是说安全阀会在更低的阈值开启,这使其与日常的葡萄糖稳态相关。目前,几种SGLT2抑制剂已被批准用于治疗肾功能正常的2型糖尿病患者。通过诱导糖尿,这些药物可改善2型糖尿病各阶段的血糖控制,而且它们导致低血糖的风险较低,因为当滤过的葡萄糖负荷降至约80克/天以下时,它们会自然停止作用,且不会干扰代谢性反调节机制。通过糖尿,SGLT2抑制剂可减轻体重和体脂,并将底物利用从碳水化合物转向脂质,甚至可能转向酮体。由于SGLT2在重吸收葡萄糖的同时也重吸收钠,SGLT2阻断剂具有利钠和降压作用。此外,由于它们作用于近端小管,SGLT2抑制剂会增加液体和电解质向致密斑的输送,从而激活管球反馈并增加肾小管内压。这可减轻肾小球高滤过,降低肾脏的需氧量,并减少蛋白尿。由于一些尚不清楚的原因,SGLT2抑制剂还具有促进尿酸排泄的作用。SGLT2抑制剂的这些多效性作用可能促成了EMPA-REG OUTCOME试验的结果,在该试验中,SGLT2抑制剂恩格列净减缓了慢性肾脏病的进展,并降低了2型糖尿病高危个体的主要不良心血管事件。本综述讨论了SGLT2在肾脏葡萄糖重吸收的生理和病理生理过程中的作用,并概述了在糖尿病肾脏中抑制SGLT2的意外逻辑。