Baron Ralf, Maier Christoph, Attal Nadine, Binder Andreas, Bouhassira Didier, Cruccu Giorgio, Finnerup Nanna B, Haanpää Maija, Hansson Per, Hüllemann Philipp, Jensen Troels S, Freynhagen Rainer, Kennedy Jeffrey D, Magerl Walter, Mainka Tina, Reimer Maren, Rice Andrew S C, Segerdahl Märta, Serra Jordi, Sindrup Sören, Sommer Claudia, Tölle Thomas, Vollert Jan, Treede Rolf-Detlef
Division of Neurological Pain Research and Therapy, Department of Neurology, Universitätsklinikum Schleswig-Holstein, Campus Kiel, Germany.
Department of Pain Medicine, BG University Hospital Bergmannsheil GmbH, Ruhr-University Bochum, Bochum, Germany.
Pain. 2017 Feb;158(2):261-272. doi: 10.1097/j.pain.0000000000000753.
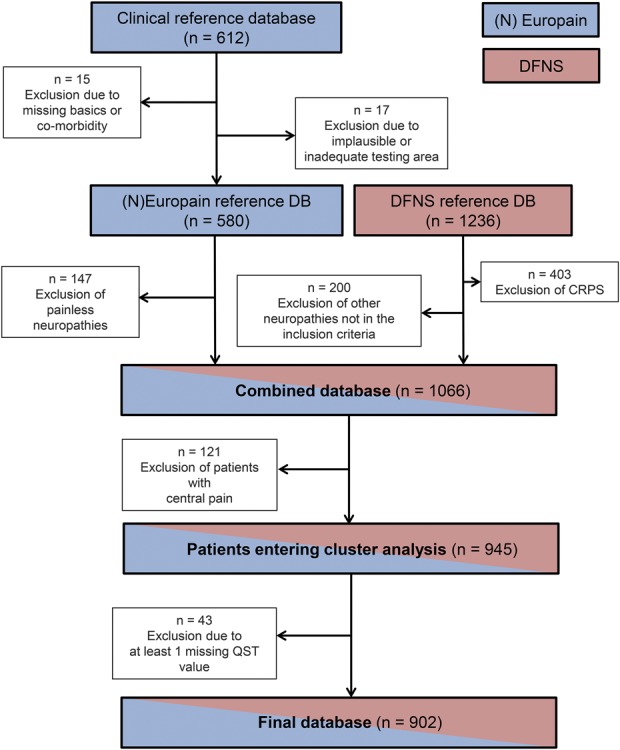
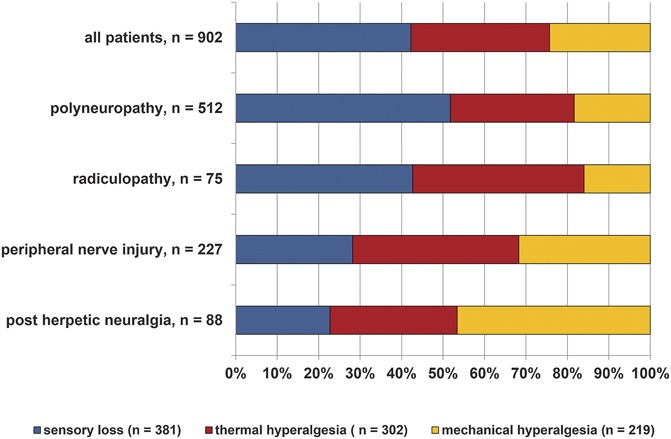
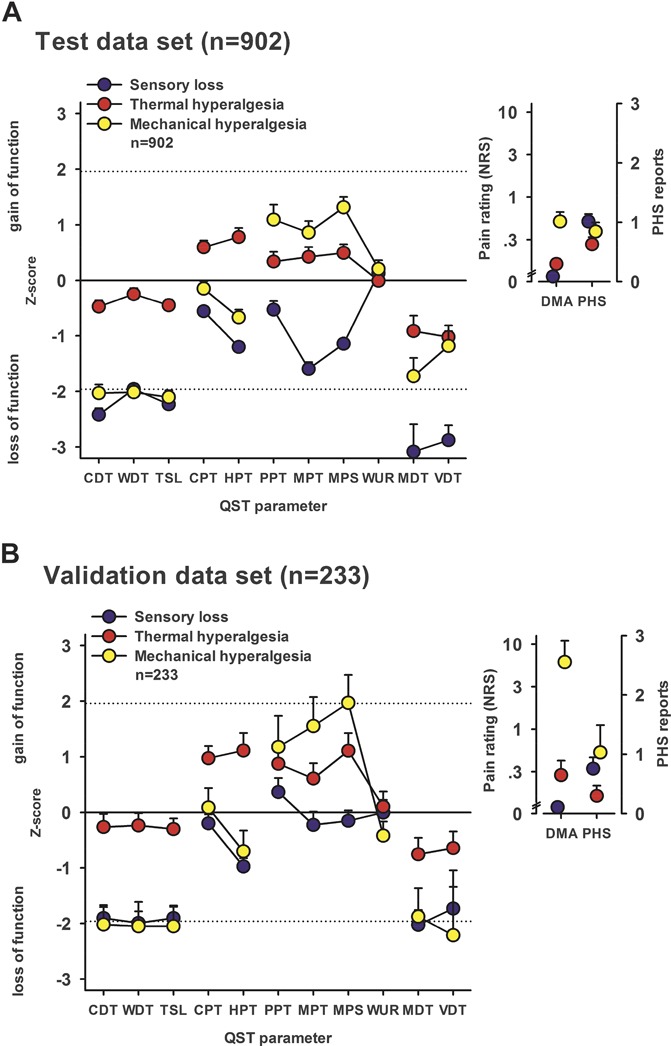
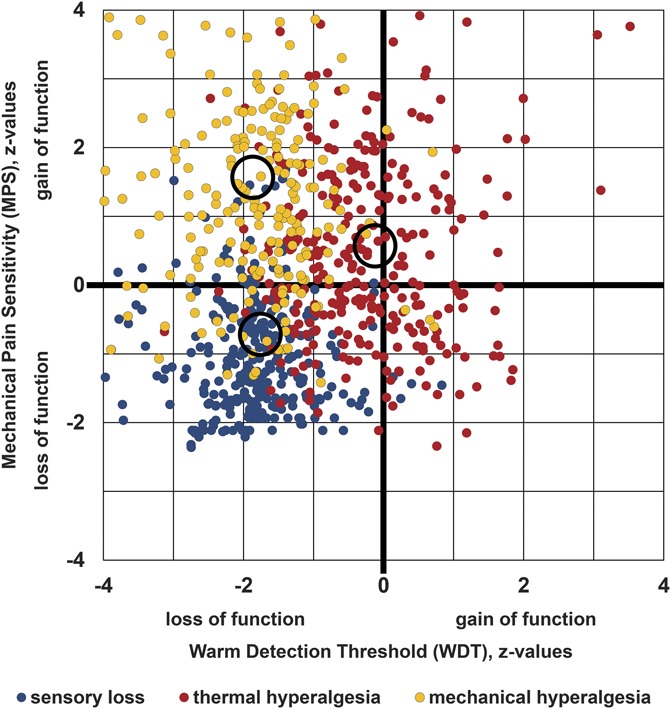
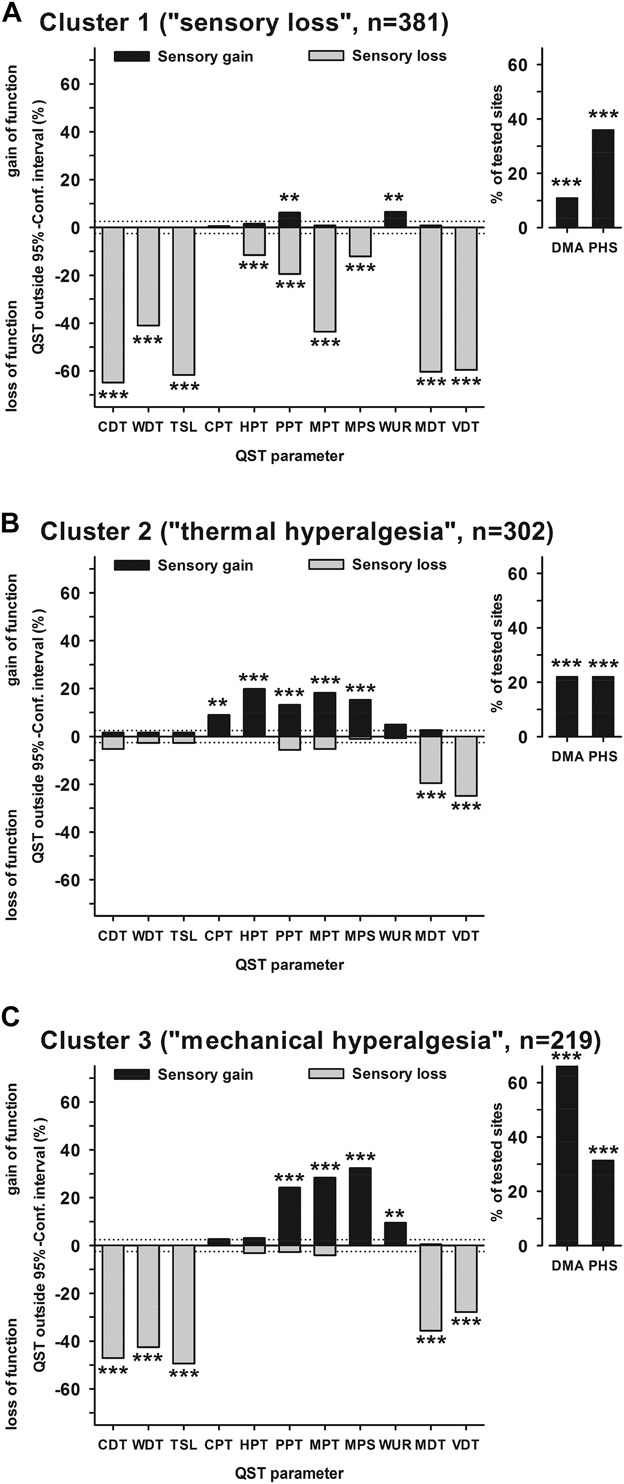
Patients with neuropathic pain are heterogeneous in etiology, pathophysiology, and clinical appearance. They exhibit a variety of pain-related sensory symptoms and signs (sensory profile). Different sensory profiles might indicate different classes of neurobiological mechanisms, and hence subgroups with different sensory profiles might respond differently to treatment. The aim of the investigation was to identify subgroups in a large sample of patients with neuropathic pain using hypothesis-free statistical methods on the database of 3 large multinational research networks (German Research Network on Neuropathic Pain (DFNS), IMI-Europain, and Neuropain). Standardized quantitative sensory testing was used in 902 (test cohort) and 233 (validation cohort) patients with peripheral neuropathic pain of different etiologies. For subgrouping, we performed a cluster analysis using 13 quantitative sensory testing parameters. Three distinct subgroups with characteristic sensory profiles were identified and replicated. Cluster 1 (sensory loss, 42%) showed a loss of small and large fiber function in combination with paradoxical heat sensations. Cluster 2 (thermal hyperalgesia, 33%) was characterized by preserved sensory functions in combination with heat and cold hyperalgesia and mild dynamic mechanical allodynia. Cluster 3 (mechanical hyperalgesia, 24%) was characterized by a loss of small fiber function in combination with pinprick hyperalgesia and dynamic mechanical allodynia. All clusters occurred across etiologies but frequencies differed. We present a new approach of subgrouping patients with peripheral neuropathic pain of different etiologies according to intrinsic sensory profiles. These 3 profiles may be related to pathophysiological mechanisms and may be useful in clinical trial design to enrich the study population for treatment responders.
神经性疼痛患者在病因、病理生理学和临床表现方面具有异质性。他们表现出各种与疼痛相关的感觉症状和体征(感觉特征)。不同的感觉特征可能表明不同类别的神经生物学机制,因此具有不同感觉特征的亚组对治疗的反应可能不同。本研究的目的是在3个大型跨国研究网络(德国神经性疼痛研究网络(DFNS)、IMI - 欧洲疼痛研究项目和神经性疼痛研究项目)的数据库中,使用无假设统计方法,在大量神经性疼痛患者样本中识别亚组。对902名(测试队列)和233名(验证队列)不同病因的周围神经性疼痛患者进行了标准化定量感觉测试。为了进行亚组划分,我们使用13个定量感觉测试参数进行了聚类分析。识别并重复验证了三个具有特征性感觉特征的不同亚组。第1组(感觉丧失,42%)表现为小纤维和大纤维功能丧失,并伴有反常热感觉。第2组(热痛觉过敏,33%)的特征是感觉功能保留,伴有热和冷痛觉过敏以及轻度动态机械性异常性疼痛。第3组(机械性痛觉过敏,24%)的特征是小纤维功能丧失,伴有针刺样痛觉过敏和动态机械性异常性疼痛。所有亚组在不同病因中均有出现,但频率有所不同。我们提出了一种根据内在感觉特征对不同病因的周围神经性疼痛患者进行亚组划分的新方法。这三种特征可能与病理生理机制相关,并且在临床试验设计中可能有助于富集治疗反应者的研究人群。