Craig Louise E, McInnes Elizabeth, Taylor Natalie, Grimley Rohan, Cadilhac Dominique A, Considine Julie, Middleton Sandy
Nursing Research Institute, St Vincent's Health Australia (Sydney) and Australian Catholic University, Sydney, NSW, Australia.
Centre for Healthcare Resilience and Implementation Science, Australian Institute of Health Innovation, Macquarie University, Sydney, NSW, Australia.
Implement Sci. 2016 Nov 28;11(1):157. doi: 10.1186/s13012-016-0524-1.
Clinical guidelines recommend that assessment and management of patients with stroke commences early including in emergency departments (ED). To inform the development of an implementation intervention targeted in ED, we conducted a systematic review of qualitative and quantitative studies to identify relevant barriers and enablers to six key clinical behaviours in acute stroke care: appropriate triage, thrombolysis administration, monitoring and management of temperature, blood glucose levels, and of swallowing difficulties and transfer of stroke patients in ED.
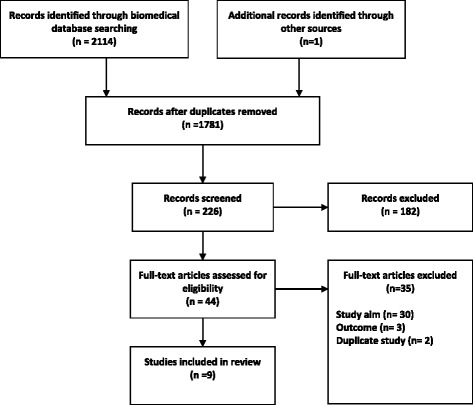
Studies of any design, conducted in ED, where barriers or enablers based on primary data were identified for one or more of these six clinical behaviours. Major biomedical databases (CINAHL, OVID SP EMBASE, OVID SP MEDLINE) were searched using comprehensive search strategies. The barriers and enablers were categorised using the theoretical domains framework (TDF). The behaviour change technique (BCT) that best aligned to the strategy each enabler represented was selected for each of the reported enablers using a standard taxonomy.
Five qualitative studies and four surveys out of the 44 studies identified met the selection criteria. The majority of barriers reported corresponded with the TDF domains of "environmental, context and resources" (such as stressful working conditions or lack of resources) and "knowledge" (such as lack of guideline awareness or familiarity). The majority of enablers corresponded with the domains of "knowledge" (such as education for physicians on the calculated risk of haemorrhage following intravenous thrombolysis [tPA]) and "skills" (such as providing opportunity to treat stroke cases of varying complexity). The total number of BCTs assigned was 18. The BCTs most frequently assigned to the reported enablers were "focus on past success" and "information about health consequences."
Barriers and enablers for the delivery of key evidence-based protocols in an emergency setting have been identified and interpreted within a relevant theoretical framework. This new knowledge has since been used to select specific BCTs to implement evidence-based care in an ED setting. It is recommended that findings from similar future reviews adopt a similar theoretical approach. In particular, the use of existing matrices to assist the selection of relevant BCTs.
临床指南建议,对中风患者的评估和管理应尽早开始,包括在急诊科(ED)。为了为针对急诊科的实施干预措施的制定提供信息,我们对定性和定量研究进行了系统评价,以确定急性中风护理中六种关键临床行为的相关障碍和促进因素:适当分诊、溶栓治疗、体温监测与管理、血糖水平监测与管理、吞咽困难监测与管理以及急诊科中风患者的转运。
在急诊科进行的任何设计的研究,其中基于原始数据确定了这六种临床行为中一种或多种的障碍或促进因素。使用综合检索策略检索主要生物医学数据库(CINAHL、OVID SP EMBASE、OVID SP MEDLINE)。使用理论领域框架(TDF)对障碍和促进因素进行分类。使用标准分类法为每个报告的促进因素选择与每个促进因素所代表的策略最相符的行为改变技术(BCT)。
44项研究中的5项定性研究和4项调查符合入选标准。报告的大多数障碍与“环境、背景和资源”(如工作压力大或资源不足)和“知识”(如缺乏指南意识或熟悉程度)的TDF领域相对应。大多数促进因素与“知识”(如对医生进行静脉溶栓(tPA)后出血计算风险的教育)和“技能”(如提供治疗不同复杂程度中风病例的机会)领域相对应。分配的BCT总数为18个。最常分配给报告的促进因素的BCT是“关注过去的成功”和“健康后果信息”。
已在相关理论框架内确定并解释了在紧急情况下实施关键循证方案的障碍和促进因素。这些新知识已被用于选择特定的BCT,以在急诊科实施循证护理。建议未来类似综述的结果采用类似的理论方法。特别是,使用现有的矩阵来协助选择相关的BCT。