Antza Christina, Stabouli Stella, Kotsis Vasilios
Hypertension Center, Third Department of Medicine, Papageorgiou Hospital.
First Department of Pediatrics, Hippokration Hospital, Aristotle University of Thessaloniki, Thessaloniki, Greece.
Vasc Health Risk Manag. 2016 Nov 15;12:443-451. doi: 10.2147/VHRM.S91020. eCollection 2016.
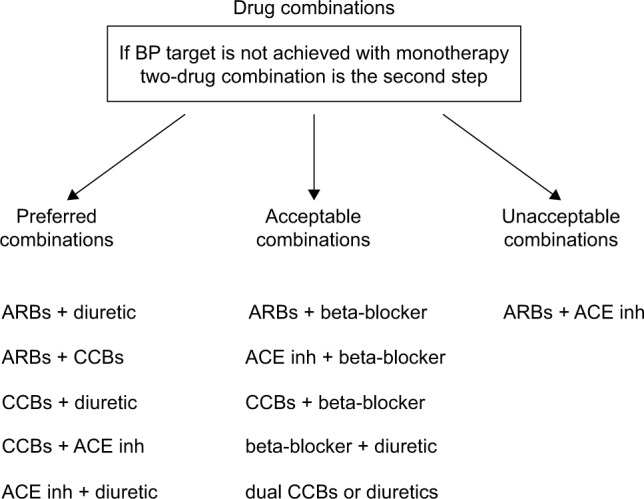
Hypertension is an important risk factor for premature death as it increases the probability of stroke, myocardial infarction, and heart failure. Antihypertensive drugs can decrease cardiovascular (CV) morbidity and mortality. The majority of hypertensive patients need more than one antihypertensive agent to attain blood pressure (BP) targets. Monotherapy can effectively reduce BP only in 20%-40% of patients. Multiple mechanisms including increased peripheral vascular resistance, increased cardiac work, and hypervolemia are involved in the pathogenesis of hypertension. Targeting multiple pathways may more potently reduce BP. Increasing the dose of a single agent in many cases does not provide the expected BP-lowering effect because the underlying mechanism of the BP increase is either different or already corrected with the lower dose. Moreover, drugs acting on different pathways may have synergistic effects and thus better control hypertension. It is well known that diuretics enhance the actions of renin-angiotensin aldosterone system and activate it as a feedback to the reduced circulated blood volume. The addition of a renin-angiotensin aldosterone system blocker to a diuretic may more effectively reduce BP because the system is upregulated. Reducing the maximal dose of an agent may also reduce possible side effects if they are dose dependent. The increased prevalence of peripheral edema with higher doses of calcium channel blockers (CCBs) is reduced when renin-angiotensin aldosterone system blockers are added to CCBs through vein dilation. The effectiveness of the combination of enalapril with lercanidipine in reducing BP, the safety profile, and the use of the combination of angiotensin-converting enzyme inhibitors with CCBs in clinical trials with excellent CV hard end point outcomes make this combination a promising therapy in the treatment of hypertension.
高血压是过早死亡的重要危险因素,因为它会增加中风、心肌梗死和心力衰竭的发生概率。抗高血压药物可降低心血管疾病(CV)的发病率和死亡率。大多数高血压患者需要不止一种抗高血压药物才能达到血压(BP)目标。单一疗法仅能使20%-40%的患者有效降低血压。高血压的发病机制涉及多种机制,包括外周血管阻力增加、心脏做功增加和血容量过多。针对多种途径可能更有效地降低血压。在许多情况下,增加单一药物的剂量并不能提供预期的降压效果,因为血压升高的潜在机制要么不同,要么已通过较低剂量得到纠正。此外,作用于不同途径的药物可能具有协同作用,从而更好地控制高血压。众所周知,利尿剂会增强肾素-血管紧张素-醛固酮系统的作用,并将其激活作为对循环血容量减少的反馈。在利尿剂中添加肾素-血管紧张素-醛固酮系统阻滞剂可能更有效地降低血压,因为该系统被上调。如果副作用与剂量相关,降低药物的最大剂量也可能减少可能的副作用。当通过静脉扩张在钙通道阻滞剂(CCB)中添加肾素-血管紧张素-醛固酮系统阻滞剂时,高剂量CCB引起的外周水肿患病率会降低。依那普利与乐卡地平联合使用在降低血压方面的有效性、安全性概况以及血管紧张素转换酶抑制剂与CCB联合使用在具有出色心血管硬终点结果的临床试验中的应用,使这种联合用药成为治疗高血压的一种有前景的疗法。