Resch Jacob E, Brown Cathleen N, Schmidt Julianne, Macciocchi Stephen N, Blueitt Damond, Cullum C Munro, Ferrara Michael S
Exercise and Sport Injury Laboratory Department of Kinesiology The University of Virginia , Charlottesville , VA.
St. Mary's Athletic Training Research Laboratory, Department of Kinesiology , University of Georgia , Athens, Georgia , USA.
BMJ Open Sport Exerc Med. 2016 Jan 19;2(1):e000012. doi: 10.1136/bmjsem-2015-000012. eCollection 2016.
A battery of clinical measures of neurocognition, balance and symptoms has been recommended for the management of sport concussion (SC) but is based on variable evidence.
To examine the sensitivity and specificity of a battery of tests to assess SC in college athletes.
Cross-sectional.
Research laboratory.
Division 1 athletes diagnosed with a SC (n=40) who were 20.2±1.60 years of age and 180.5±11.12 cm tall and healthy athletes (n=40) who were 19.0±0.93 years of age and 179.1±11.39 cm tall were enrolled.
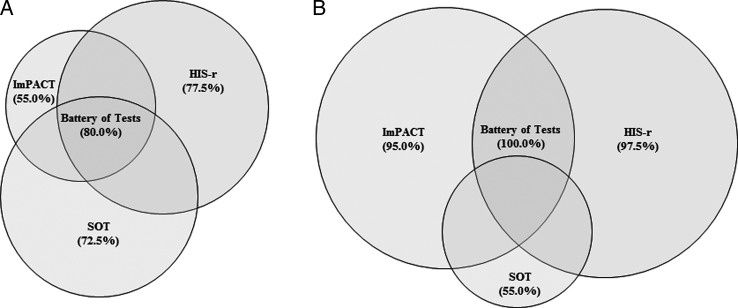
Participants were administered Immediate Postconcussion Assessment and Cognitive Test (ImPACT), the Sensory Organization Test (SOT) and the Revised Head Injury Scale (HIS-r) prior to and up to 24 h following injury between the 2004 and 2014 sport seasons. Sensitivity and specificity were calculated using predictive discriminant analyses (PDA) and clinical interpretation guidelines.
Outcome measures included baseline and postinjury ImPACT, SOT and HIS-r composite scores.
Using PDA, each clinical measure's sensitivity ranged from 55.0% to 77.5% and specificity ranged from 52.5% to 100%. The test battery possessed a sensitivity and specificity of 80.0% and 100%, respectively. Using clinical interpretation guidelines, sensitivity ranged from 55% to 97.5% individually, and 100% when combined.
Our results support a multidimensional approach to assess SC in college athletes which correctly identified 80-100% of concussed participants as injured. When each test was evaluated separately, up to 47.5% of our sample was misclassified. Caution is warranted when using singular measures to manage SC.
一系列用于管理运动性脑震荡(SC)的神经认知、平衡和症状的临床测量方法已被推荐,但所依据的证据并不一致。
检验一组测试评估大学生运动员运动性脑震荡的敏感性和特异性。
横断面研究。
研究实验室。
招募了1组被诊断为运动性脑震荡的运动员(n = 40),年龄为20.2±1.60岁,身高为180.5±11.12厘米,以及健康运动员(n = 40),年龄为19.0±0.93岁,身高为179.1±11.39厘米。
在2004年至2014年运动赛季期间,在受伤前及受伤后24小时内,对参与者进行即刻脑震荡后评估和认知测试(ImPACT)、感觉组织测试(SOT)和修订的头部损伤量表(HIS-r)。使用预测判别分析(PDA)和临床解释指南计算敏感性和特异性。
观察指标包括基线和伤后ImPACT、SOT和HIS-r综合评分。
使用PDA,每项临床测量的敏感性范围为55.0%至77.5%,特异性范围为52.5%至100%。该测试组合的敏感性和特异性分别为80.0%和100%。使用临床解释指南时,个体敏感性范围为55%至97.5%,组合时为100%。
我们的结果支持采用多维度方法评估大学生运动员的运动性脑震荡,该方法能正确识别80%-100%的脑震荡参与者为受伤。当分别评估每项测试时,我们样本中高达47.5%被错误分类。使用单一测量方法管理运动性脑震荡时需谨慎。