Villafranca Alexander, Hamlin Colin, Enns Stephanie, Jacobsohn Eric
Department of Anesthesia & Perioperative Medicine, Max Rady College of Medicine, Rady Faculty of Health Sciences, University of Manitoba, 2nd Floor, Harry Medovy House, 671 William Ave, Winnipeg, MB, R3E 0Z2, Canada.
Can J Anaesth. 2017 Feb;64(2):128-140. doi: 10.1007/s12630-016-0784-x. Epub 2016 Nov 29.
Disruptive behaviour, which we define as behaviour that does not show others an adequate level of respect and causes victims or witnesses to feel threatened, is a concern in the operating room. This review summarizes the current literature on disruptive behaviour as it applies to the perioperative domain.
Searches of MEDLINE, Scopus™, and Google books identified articles and monographs of interest, with backreferencing used as a supplemental strategy.
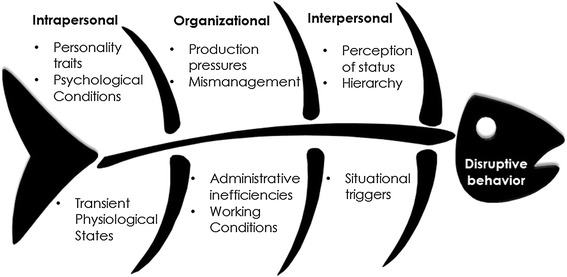
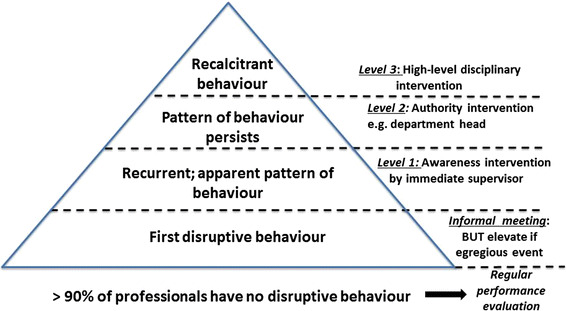
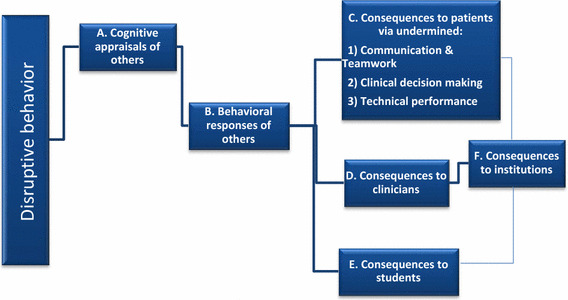
Much of the data comes from studies outside the operating room and has significant methodological limitations. Disruptive behaviour has intrapersonal, interpersonal, and organizational causes. While fewer than 10% of clinicians display disruptive behaviour, up to 98% of clinicians report witnessing disruptive behaviour in the last year, 70% report being treated with incivility, and 36% report being bullied. This type of conduct can have many negative ramifications for clinicians, students, and institutions. Although the evidence regarding patient outcomes is primarily based on clinician perceptions, anecdotes, and expert opinion, this evidence supports the contention of an increase in morbidity and mortality. The plausible mechanism for this increase is social undermining of teamwork, communication, clinical decision-making, and technical performance. The behavioural responses of those who are exposed to such conduct can positively or adversely moderate the consequences of disruptive behaviour. All operating room professions are involved, with the rank order (from high to low) being surgeons, nurses, anesthesiologists, and "others". The optimal approaches to the prevention and management of disruptive behaviour are uncertain, but they include preventative and professional development courses, training in soft skills and teamwork, institutional efforts to optimize the workplace, clinician contracts outlining the clinician's (and institution's) responsibilities, institutional policies that are monitored and enforced, regular performance feedback, and clinician coaching/remediation as required.
Disruptive behaviour remains a part of operating room culture, with many associated deleterious effects. There is a widely accepted view that disruptive behaviour can lead to increased patient morbidity and mortality. This is mechanistically plausible, but more rigorous studies are required to confirm the effects and estimate their magnitude. An important measure that individual clinicians can take is to monitor and control their own behaviour, including their responses to disruptive behaviour.
破坏性行为,即我们定义的未向他人展现出足够尊重程度并使受害者或目击者感到受到威胁的行为,是手术室中令人担忧的问题。本综述总结了当前适用于围手术期领域的关于破坏性行为的文献。
检索MEDLINE、Scopus™和谷歌图书,确定感兴趣的文章和专著,并将回溯参考文献作为补充策略。
大部分数据来自手术室以外的研究,且存在显著的方法学局限性。破坏性行为具有个人、人际和组织方面的成因。虽然不到10%的临床医生表现出破坏性行为,但高达98%的临床医生报告在过去一年中目睹过破坏性行为,70%报告受到过无礼对待,36%报告遭受过欺凌。这种行为会给临床医生、学生和机构带来许多负面影响。尽管关于患者结局的证据主要基于临床医生的看法、轶事和专家意见,但这些证据支持发病率和死亡率上升这一观点。这种上升的合理机制是对团队合作、沟通、临床决策和技术操作的社会破坏。遭受此类行为的人的行为反应可以积极或消极地缓和破坏性行为的后果。手术室的所有职业都涉及其中,发生率排序(从高到低)为外科医生、护士、麻醉医生和“其他人员”。预防和管理破坏性行为的最佳方法尚不确定,但包括预防性和专业发展课程、软技能和团队合作培训、机构优化工作场所的努力、概述临床医生(和机构)责任的临床医生合同、受到监督和执行的机构政策、定期绩效反馈以及根据需要进行的临床医生辅导/纠正。
破坏性行为仍是手术室文化的一部分,具有许多相关的有害影响。人们普遍认为破坏性行为会导致患者发病率和死亡率上升。这在机制上是合理的,但需要更严格的研究来证实其影响并估计其程度。临床医生个人可以采取的一项重要措施是监测和控制自己的行为,包括对破坏性行为的反应。