Ainsworth B, Steele M, Stuart B, Joseph J, Miller S, Morrison L, Little P, Yardley L
Centre for Clinical and Community Applications of Health Psychology, Psychology, Faculty of Social and Human Sciences, University of Southampton, Southampton, SO17 1BJ, UK.
Primary Care and Population Sciences, Faculty of Medicine, University of Southampton, Southampton, UK.
Ann Behav Med. 2017 Jun;51(3):423-431. doi: 10.1007/s12160-016-9866-9.
In designing digital interventions for healthcare, it is important to understand not just whether interventions work but also how and for whom-including whether individual intervention components have different effects, whether a certain usage threshold is required to change behavior in each intervention and whether usage differs across population subgroups.
We investigated these questions using data from a large trial of the digital PRimary care trial of a website based Infection control intervention to Modify Influenza-like illness and respiratory tract infection Transmission) (PRIMIT) intervention, which aimed to reduce respiratory tract infections (RTIs) by increasing hand hygiene behavior.
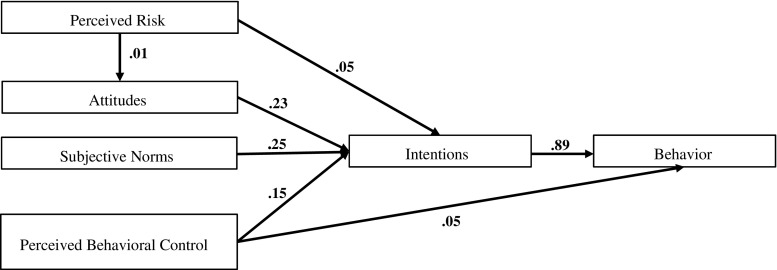
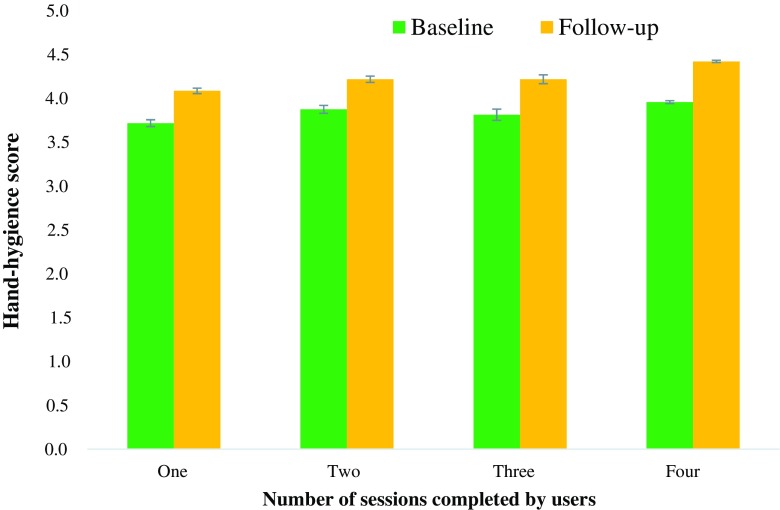
Baseline and follow-up questionnaires measured behaviors, intentions and attitudes in hand hygiene. In conjunction with objective measures of usage of the four PRIMIT sessions, we analysed these observational data to examine mechanisms of behavior change in 8993 intervention users.
We found that the PRIMIT intervention changed behavior, intentions and attitudes, and this change was associated with reduced RTIs. The largest hand hygiene change occurred after the first session, with incrementally smaller changes after each subsequent session, suggesting that engagement with the core behavior change techniques included in the first session was necessary and sufficient for behavior change. The intervention was equally effective for men and women, older and younger people and was particularly effective for those with lower levels of education.
Our well-powered analysis has implications for intervention development. We were able to determine a 'minimum threshold' of intervention engagement that is required for hand hygiene change, and we discuss the potential implications this (and other analyses of this type) may have for further intervention development. We also discuss the application of similar analyses to other interventions.
在设计医疗保健领域的数字干预措施时,重要的不仅是了解干预措施是否有效,还包括其作用方式以及对哪些人有效——包括各个干预组成部分是否有不同效果、每种干预措施改变行为是否需要一定的使用阈值,以及不同人群亚组的使用情况是否存在差异。
我们利用一项大型试验的数据来研究这些问题,该试验是关于基于网站的感染控制干预措施以改变流感样疾病和呼吸道感染传播的数字初级保健试验(PRIMIT)干预,其旨在通过增加手部卫生行为来减少呼吸道感染(RTIs)。
基线和随访问卷测量了手部卫生方面的行为、意图和态度。结合对PRIMIT四个环节使用情况的客观测量,我们分析了这些观察数据,以研究8993名干预使用者的行为改变机制。
我们发现PRIMIT干预改变了行为、意图和态度,且这种改变与呼吸道感染减少相关。最大的手部卫生改变发生在第一个环节之后,随后每个环节的改变逐渐变小,这表明参与第一个环节中包含的核心行为改变技巧对于行为改变是必要且充分的。该干预措施对男性和女性、老年人和年轻人同样有效,对教育程度较低的人尤其有效。
我们有力的分析对干预措施的开发具有启示意义。我们能够确定手部卫生改变所需的干预参与“最低阈值”,并讨论了这一点(以及此类其他分析)对进一步干预开发可能产生的潜在影响。我们还讨论了类似分析在其他干预措施中的应用。