Mason John D, Blencowe Natalie S, McNair Angus Gk, Stevens Daniel J, Avery Kerry N, Pullyblank Anne M, Blazeby Jane M
Centre for Surgical Research, School of Social and Community Medicine, University of Bristol, Canynge Hall, 39 Whatley Road, Bristol, BS8 2PS UK.
Centre for Surgical Research, School of Social and Community Medicine, University of Bristol, Canynge Hall, 39 Whatley Road, Bristol, BS8 2PS UK ; Division of Surgery, Head and Neck, University Hospitals Bristol NHS Foundation Trust, Bristol Royal Infirmary, Marlborough Street, Bristol, BS2 8HW UK.
Pilot Feasibility Stud. 2015 May 9;1:16. doi: 10.1186/s40814-015-0011-5. eCollection 2015.
Randomised controlled trials (RCTs) in surgery can be challenging to conduct, and trials in the emergency surgical setting when patients have unplanned hospital admissions are particularly difficult. One area of challenge is capturing baseline patient-reported outcome (PRO) data. This study examined the feasibility and optimal methods for the collection of baseline and follow-up PRO data in the setting of unplanned surgical hospital admissions.
Clinically stable adult patients with unplanned admissions through the day and night under the care of general surgeons at two acute NHS trusts were approached during working week days and asked to complete validated PRO measures (European Quality of Life-5 Dimension, Short Form-12, and Gastrointestinal Quality of Life Index) on admission and 6 weeks following discharge. Feasibility of PRO data collection was determined by the proportions of admitted patients eligible and recruited and by questionnaire-response rates at baseline and follow up. Reasons for non-recruitment and non-completion of questionnaires were sought and recorded.
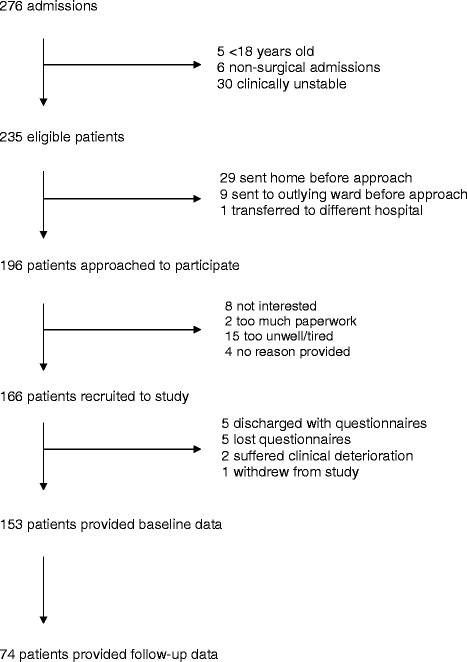
There were 276 admissions, of whom 235 (85.1 %) were eligible. Reasons for ineligibility were the following: age under 18 years old ( = 5, 1.8 %), non-surgical presenting complaint ( = 6, 2.2 %) and clinical instability ( = 30, 10.9 %). One hundred and sixty-six patients (70.6 %) were recruited (98 female, 59.0 %); median age 53, range 19-100). Common reasons for non-recruitment included patients being discharged home before approached by researchers ( = 29, 12.3 %) or declining participation because they felt unwell ( = 15, 6.4 %). The most common reason for admission to the hospital was abdominal pain ( = 120, 72.3 % recruited patients), of whom 50 (30.1 %) required operative intervention. Baseline PRO data was obtained from 153 patients (93.3 %), and 74 (48.4 %) returned follow-up questionnaires.
Collection of baseline PRO data amongst unplanned admissions in general surgery is feasible. Methods for optimising retention and follow up are needed.
外科领域的随机对照试验(RCTs)实施起来可能具有挑战性,而针对患者非计划入院的急诊外科环境下的试验尤其困难。其中一个挑战领域是获取患者报告的基线结局(PRO)数据。本研究探讨了在非计划外科住院情况下收集基线和随访PRO数据的可行性及最佳方法。
在两个急性国民保健服务(NHS)信托机构中,工作日期间对在普通外科医生照料下日间和夜间非计划入院的临床稳定成年患者进行询问,要求他们在入院时及出院后6周完成经过验证的PRO测量(欧洲生活质量五维度量表、简明健康调查问卷12项版和胃肠道生活质量指数)。通过符合条件并被招募的入院患者比例以及基线和随访时的问卷回复率来确定PRO数据收集的可行性。寻找并记录未被招募和未完成问卷的原因。
共有276例入院患者,其中235例(85.1%)符合条件。不符合条件的原因如下:年龄不满18岁(n = 5,1.8%)、非手术主诉(n = 6,2.2%)和临床不稳定(n = 30,10.9%)。166例患者(70.6%)被招募(98例女性,59.0%);年龄中位数53岁,范围19 - 100岁)。未被招募的常见原因包括患者在研究人员询问之前已出院回家(n = 29,12.3%)或因感觉不适而拒绝参与(n = 15,6.4%)。入院的最常见原因是腹痛(n = 120,72.3%的被招募患者),其中50例(30.1%)需要手术干预。从153例患者(93.3%)获得了基线PRO数据,74例(48.4%)返回了随访问卷。
在普通外科非计划入院患者中收集基线PRO数据是可行的。需要优化留存率和随访的方法。