School of Health and Related Research (ScHARR), University of Sheffield, Sheffield, UK.
Health Qual Life Outcomes. 2012 Feb 3;10:20. doi: 10.1186/1477-7525-10-20.
Health utility combines health related quality of life and mortality to produce a generic outcome measure reflecting both morbidity and mortality. It has not been widely used as an outcome measure in evaluations of emergency care and little is known about the feasibility of measurement, typical values obtained or baseline factors that predict health utility. We aimed to measure health utility after emergency medical admission, to compare health utility to age, gender and regional population norms, and identify independent predictors of health utility.
We selected 5760 patients across three hospitals who were admitted to hospital by ambulance as a medical emergency. The EQ-5D questionnaire was mailed to all who were still alive 30 days after admission. Health utility was estimated by applying tariff values to the EQ-5D responses or imputing a value of zero for those who had died. Multivariable analysis was used to identify independent predictors of health utility at 30 days.
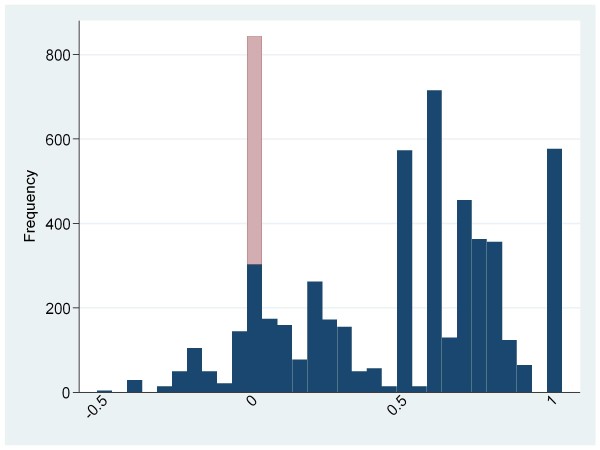
Responses were received from 2488 (47.7%) patients, while 541 (9.4%) had died. Most respondents reported some or severe problems with each aspect of health. Mean health utility was 0.49 (standard deviation 0.35) in survivors and 0.45 (0.36) including non-survivors. Some 75% had health utility below their expected value (mean loss 0.32, 95% confidence interval 0.31 to 0.33) and 11% had health utility below zero (worse than death). On multivariable modelling, reduced health utility was associated with increased age and lower GCS, varied according to ICD10 code and was lower among females, patients with recent hospital admission, steroid therapy, or history of chronic respiratory disease, malignancy, diabetes or epilepsy.
Health utility can be measured after emergency medical admission, although responder bias may be significant. Health utility after emergency medical admission is poor compared to population norms. We have identified independent predictors or health utility that need to be measured and taken into account in non-randomized evaluations of emergency care.
健康效用将健康相关生活质量和死亡率结合起来,生成一个反映发病率和死亡率的通用结果测量指标。它尚未广泛用作急诊护理评估的结果测量指标,对其测量的可行性、获得的典型值或预测健康效用的基线因素知之甚少。我们旨在测量急诊入院后的健康效用,将健康效用与年龄、性别和地区人群正常值进行比较,并确定健康效用的独立预测因素。
我们在三家医院中选择了 5760 名因医疗紧急情况被救护车送往医院的患者。在入院 30 天后,向所有仍存活的患者邮寄 EQ-5D 问卷。通过将关税值应用于 EQ-5D 响应或为已死亡的患者输入零值,来估算健康效用。使用多变量分析来确定 30 天时健康效用的独立预测因素。
共收到 2488 名(47.7%)患者的回复,其中 541 名(9.4%)患者死亡。大多数受访者报告在健康的各个方面都存在一些或严重的问题。幸存者的平均健康效用为 0.49(标准差 0.35),包括非幸存者在内为 0.45(0.36)。约 75%的患者健康效用低于预期值(平均损失 0.32,95%置信区间 0.31 至 0.33),11%的患者健康效用低于零(比死亡更糟)。在多变量建模中,健康效用降低与年龄增加和格拉斯哥昏迷量表(GCS)降低相关,因 ICD10 代码而异,在女性、近期住院、类固醇治疗或有慢性呼吸系统疾病、恶性肿瘤、糖尿病或癫痫病史的患者中较低。
可以在急诊医疗入院后测量健康效用,尽管应答者偏倚可能很大。与人群正常值相比,急诊医疗入院后的健康效用较差。我们已经确定了健康效用的独立预测因素,需要在非随机急诊护理评估中进行测量并加以考虑。