Nacu Aliona, Kvistad Christopher E, Naess Halvor, Øygarden Halvor, Logallo Nicola, Assmus Jörg, Waje-Andreassen Ulrike, Kurz Kathinka D, Neckelmann Gesche, Thomassen Lars
From the Department of Neurology (A.N., C.E.K., H.N., H.Ø., N.L., U.W.-A., L.T.) and Department of Radiology (G.N.), Haukeland University Hospital, Bergen, Norway; Department of Clinical Medicine (A.N., H.N., H.Ø., L.T.) and Department of Biostatistics (J.A.), University of Bergen, Norway; and Center for Age-Related Medicine (H.N.) and Department of Radiology (K.D.K.), Stavanger University Hospital, Norway.
Stroke. 2017 Feb;48(2):335-341. doi: 10.1161/STROKEAHA.116.014644. Epub 2016 Dec 15.
The NOR-SASS (Norwegian Sonothrombolysis in Acute Stroke Study) aimed to assess effect and safety of contrast-enhanced ultrasound treatment in an unselected acute ischemic stroke population.
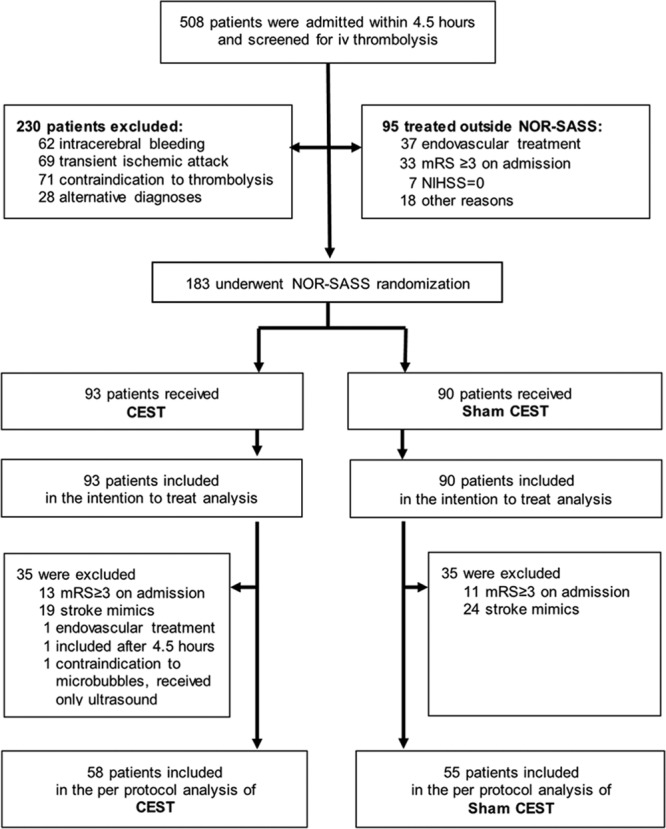
Patients treated with intravenous thrombolysis within 4.5 hours after symptom onset were randomized 1:1 to either contrast-enhanced sonothrombolysis (CEST) or sham CEST. A visible arterial occlusion on baseline computed tomography angiography was not a prerequisite for inclusion. Pulse-wave 2 MHz ultrasound was given for 1 hour and contrast (SonoVue) as an infusion for ≈30 minutes. Magnetic resonance imaging and angiography were performed after 24 to 36 hours. Primary study end points were neurological improvement at 24 hours defined as National Institutes of Health Stroke Scale score 0 or reduction of ≥4 National Institutes of Health Stroke Scale points compared with baseline National Institutes of Health Stroke Scale and favorable functional outcome at 90 days defined as modified Rankin scale score 0 to 1.
A total of 183 patients were randomly assigned to either CEST (93 patient) or sham CEST (90 patients). The rates of symptomatic intracerebral hemorrhage, asymptomatic intracerebral hemorrhage, or mortality were not increased in the CEST group. Neurological improvement at 24 hours and functional outcome at 90 days was similar in the 2 groups both in the intention-to-treat analysis and in the per-protocol analysis.
CEST is safe among unselected ischemic stroke patients with or without a visible occlusion on computed tomography angiography and with varying grades of clinical severity. There was, however, statistically no significant clinical effect of sonothrombolysis in this prematurely stopped trial.
URL: http://www.clinicaltrials.gov. Unique identifier: NCT01949961.
挪威急性卒中超声溶栓研究(NOR-SASS)旨在评估在未选择的急性缺血性卒中患者群体中,超声造影增强治疗的效果和安全性。
症状发作后4.5小时内接受静脉溶栓治疗的患者按1:1随机分为超声造影增强溶栓治疗(CEST)组或假CEST组。基线计算机断层扫描血管造影显示可见动脉闭塞并非纳入研究的必要条件。给予2兆赫脉冲波超声治疗1小时,并静脉输注造影剂(声诺维)约30分钟。在24至36小时后进行磁共振成像和血管造影。主要研究终点为24小时时的神经功能改善,定义为美国国立卫生研究院卒中量表(NIHSS)评分0或与基线NIHSS评分相比NIHSS评分降低≥4分,以及90天时良好的功能结局,定义为改良Rankin量表评分0至1分。
共有183例患者被随机分配至CEST组(93例患者)或假CEST组(90例患者)。CEST组有症状性脑出血、无症状性脑出血或死亡率均未增加。在意向性分析和符合方案分析中,两组在24小时时的神经功能改善和90天时的功能结局相似。
在未选择的缺血性卒中患者中,无论计算机断层扫描血管造影上有无可见闭塞以及临床严重程度如何,CEST都是安全的。然而,在这项提前终止的试验中,超声溶栓在统计学上没有显著的临床效果。