Chouhan Manil D, Bainbridge Alan, Atkinson David, Punwani Shonit, Mookerjee Rajeshwar P, Lythgoe Mark F, Taylor Stuart A
Division of Medicine, University College London (UCL) Centre for Medical Imaging, UCL, London, UK.
Phys Med Biol. 2017 Feb 21;62(4):1533-1546. doi: 10.1088/1361-6560/aa553c. Epub 2016 Dec 21.
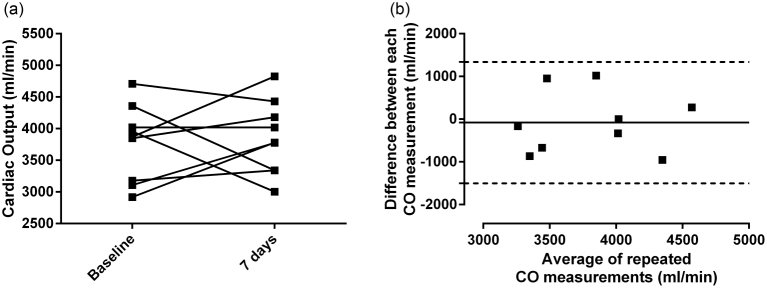
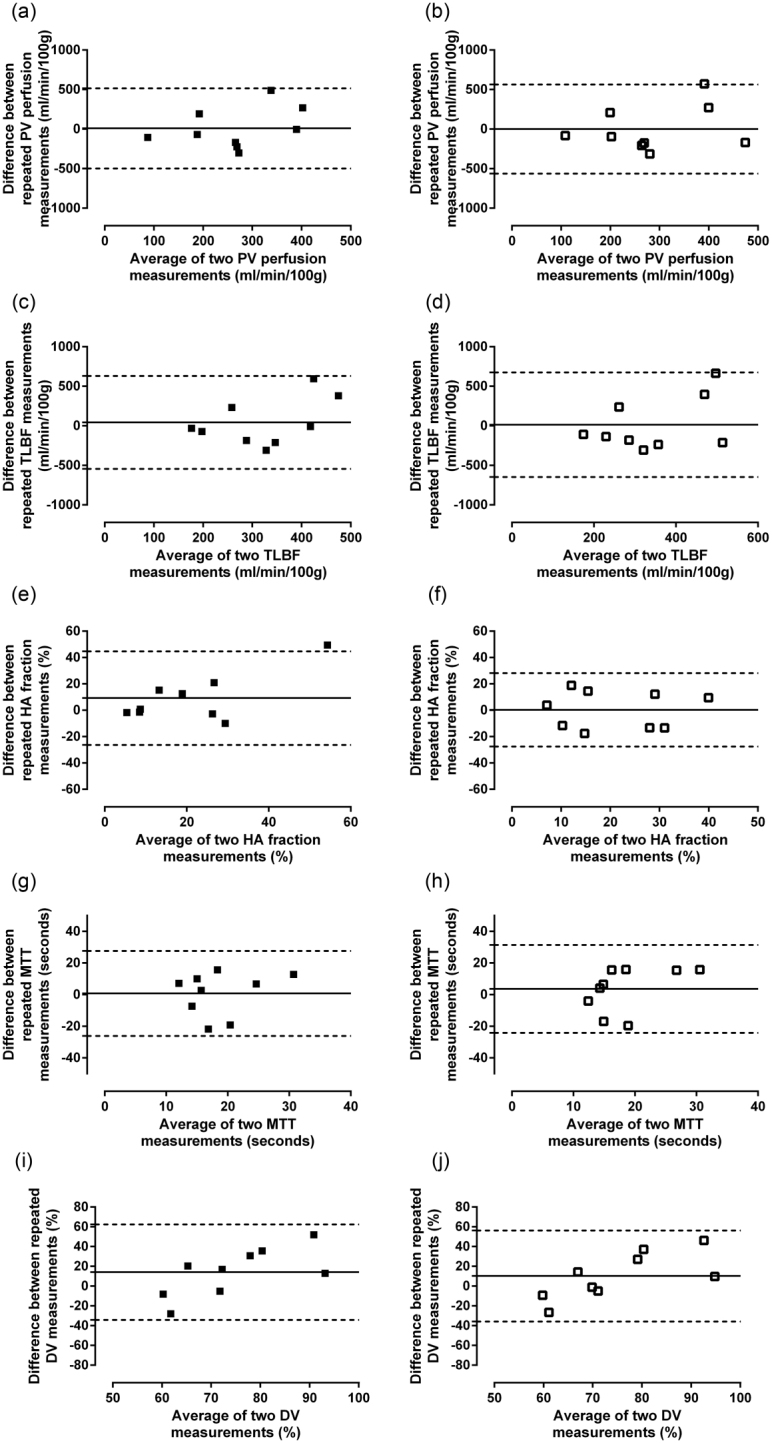
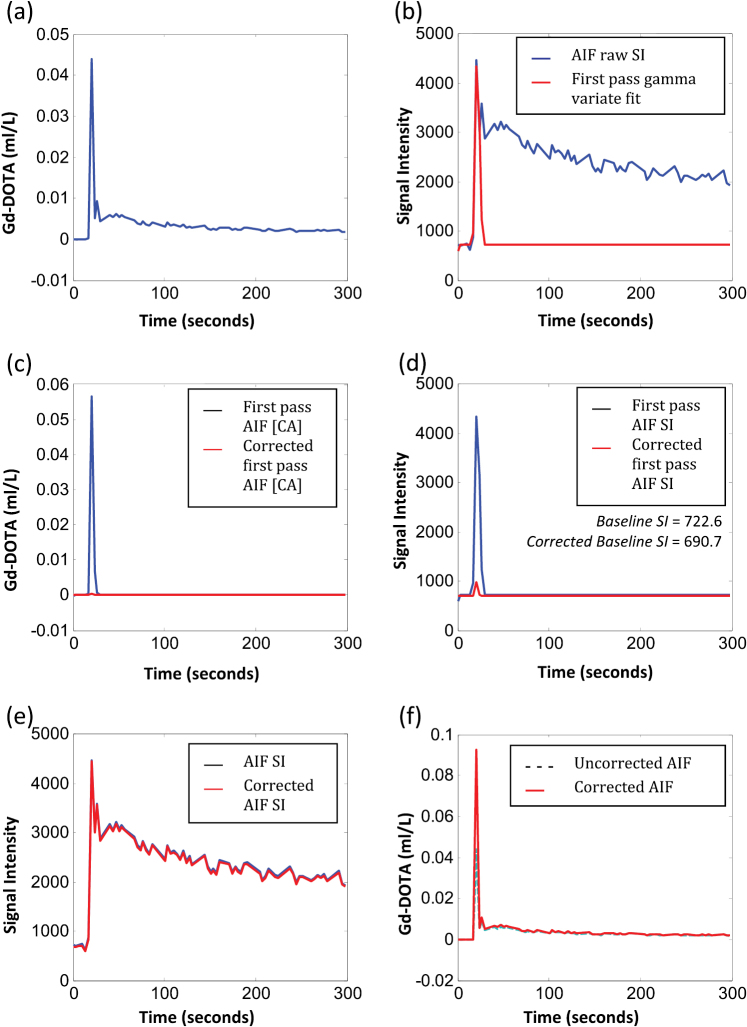
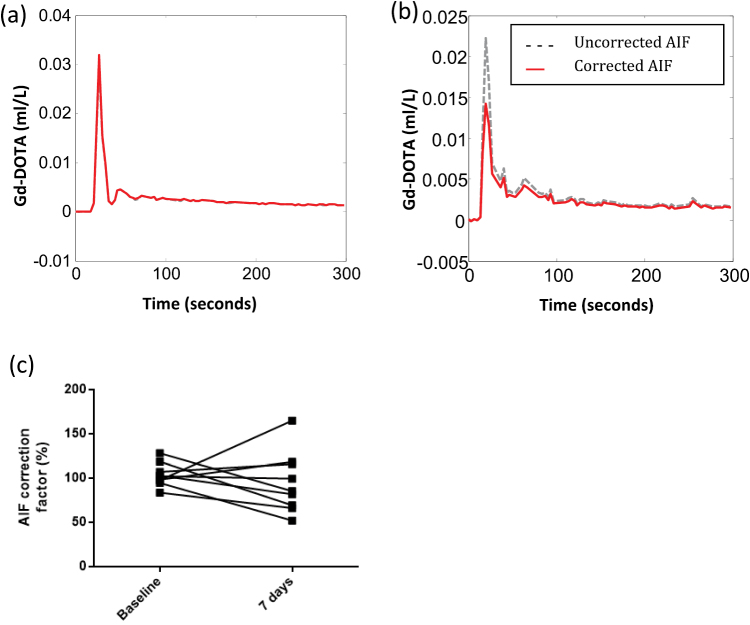
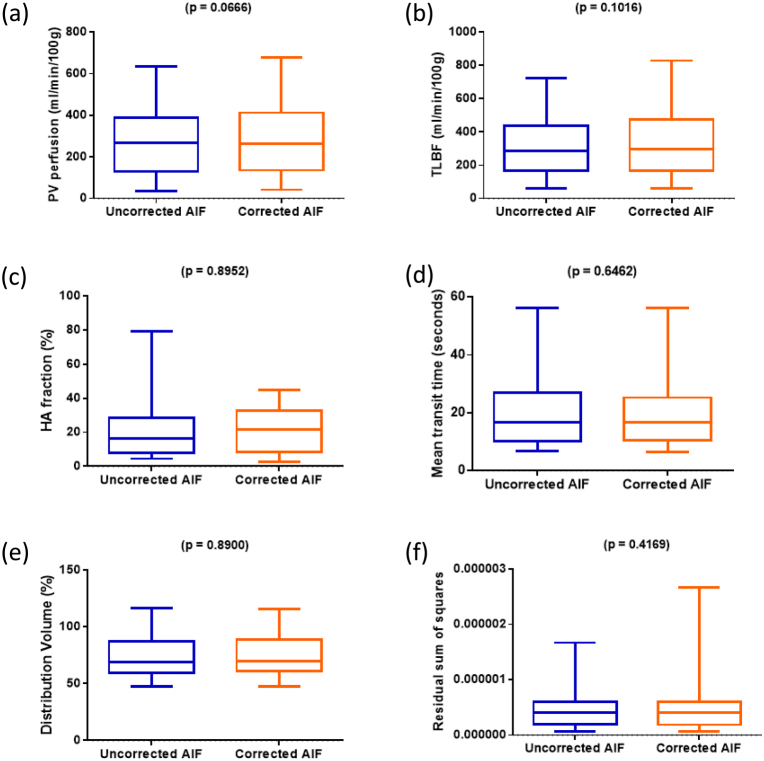
Liver dynamic contrast enhanced (DCE) MRI pharmacokinetic modelling could be useful in the assessment of diffuse liver disease and focal liver lesions, but is compromised by errors in arterial input function (AIF) sampling. In this study, we apply cardiac output correction to arterial input functions (AIFs) for liver DCE MRI and investigate the effect on dual-input single compartment hepatic perfusion parameter estimation and reproducibility. Thirteen healthy volunteers (28.7 ± 1.94 years, seven males) underwent liver DCE MRI and cardiac output measurement using aortic root phase contrast MRI (PCMRI), with reproducibility (n = 9) measured at 7 d. Cardiac output AIF correction was undertaken by constraining the first pass AIF enhancement curve using the indicator-dilution principle. Hepatic perfusion parameters with and without cardiac output AIF correction were compared and 7 d reproducibility assessed. Differences between cardiac output corrected and uncorrected liver DCE MRI portal venous (PV) perfusion (p = 0.066), total liver blood flow (TLBF) (p = 0.101), hepatic arterial (HA) fraction (p = 0.895), mean transit time (MTT) (p = 0.646), distribution volume (DV) (p = 0.890) were not significantly different. Seven day corrected HA fraction reproducibility was improved (mean difference 0.3%, Bland-Altman 95% limits-of-agreement (BA95%LoA) ±27.9%, coefficient of variation (CoV) 61.4% versus 9.3%, ±35.5%, 81.7% respectively without correction). Seven day uncorrected PV perfusion was also improved (mean difference 9.3 ml min/100 g, BA95%LoA ±506.1 ml min/100 g, CoV 64.1% versus 0.9 ml min/100 g, ±562.8 ml min/100 g, 65.1% respectively with correction) as was uncorrected TLBF (mean difference 43.8 ml min/100 g, BA95%LoA ±586.7 ml min/ 100 g, CoV 58.3% versus 13.3 ml min/100 g, ±661.5 ml min/100 g, 60.9% respectively with correction). Reproducibility of uncorrected MTT was similar (uncorrected mean difference 2.4 s, BA95%LoA ±26.7 s, CoV 60.8% uncorrected versus 3.7 s, ±27.8 s, 62.0% respectively with correction), as was and DV (uncorrected mean difference 14.1%, BA95%LoA ±48.2%, CoV 24.7% versus 10.3%, ±46.0%, 23.9% respectively with correction). Cardiac output AIF correction does not significantly affect the estimation of hepatic perfusion parameters but demonstrates improvements in normal volunteer 7 d HA fraction reproducibility, but deterioration in PV perfusion and TLBF reproducibility. Improved HA fraction reproducibility maybe important as arterialisation of liver perfusion is increased in chronic liver disease and within malignant liver lesions.
肝脏动态对比增强(DCE)磁共振成像(MRI)的药代动力学建模在弥漫性肝病和肝脏局灶性病变的评估中可能有用,但受到动脉输入函数(AIF)采样误差的影响。在本研究中,我们对肝脏DCE MRI的动脉输入函数(AIF)应用心输出量校正,并研究其对双输入单室肝灌注参数估计及可重复性的影响。13名健康志愿者(28.7±1.94岁,7名男性)接受了肝脏DCE MRI检查,并使用主动脉根部相位对比MRI(PCMRI)测量心输出量,在第7天测量可重复性(n = 9)。通过使用指示剂稀释原理约束首过AIF增强曲线来进行心输出量AIF校正。比较了校正和未校正心输出量AIF时的肝灌注参数,并评估了第7天的可重复性。校正和未校正心输出量的肝脏DCE MRI门静脉(PV)灌注(p = 0.066)、全肝血流量(TLBF)(p = 0.101)、肝动脉(HA)分数(p = 0.895)、平均通过时间(MTT)(p = 0.646)、分布容积(DV)(p = 0.890)之间的差异无统计学意义。校正后第7天HA分数的可重复性有所改善(平均差异0.3%,Bland-Altman 95%一致性界限(BA95%LoA)±27.9%,变异系数(CoV)分别为61.4%和9.3%,未校正时分别为±35.5%、81.7%)。未校正的第7天PV灌注也有所改善(平均差异9.3 ml·min/100 g,BA95%LoA±506.1 ml·min/100 g,CoV分别为64.1%和0.9 ml·min/100 g,校正后分别为±562.8 ml·min/100 g、65.1%),未校正的TLBF也是如此(平均差异43.8 ml·min/100 g,BA95%LoA±