Center for Outcomes Research and Evaluation, Yale-New Haven Hospital, New Haven, Connecticut.
Section of Cardiovascular Medicine, Department of Medicine, Yale School of Medicine, New Haven, Connecticut.
JAMA Netw Open. 2018 Oct 5;1(6):e183519. doi: 10.1001/jamanetworkopen.2018.3519.
Payers and policy makers have advocated for transitioning toward value-based payment models. However, little is known about what is the extent of hospital variation in the value of care and whether there are any hospital characteristics associated with high-value care.
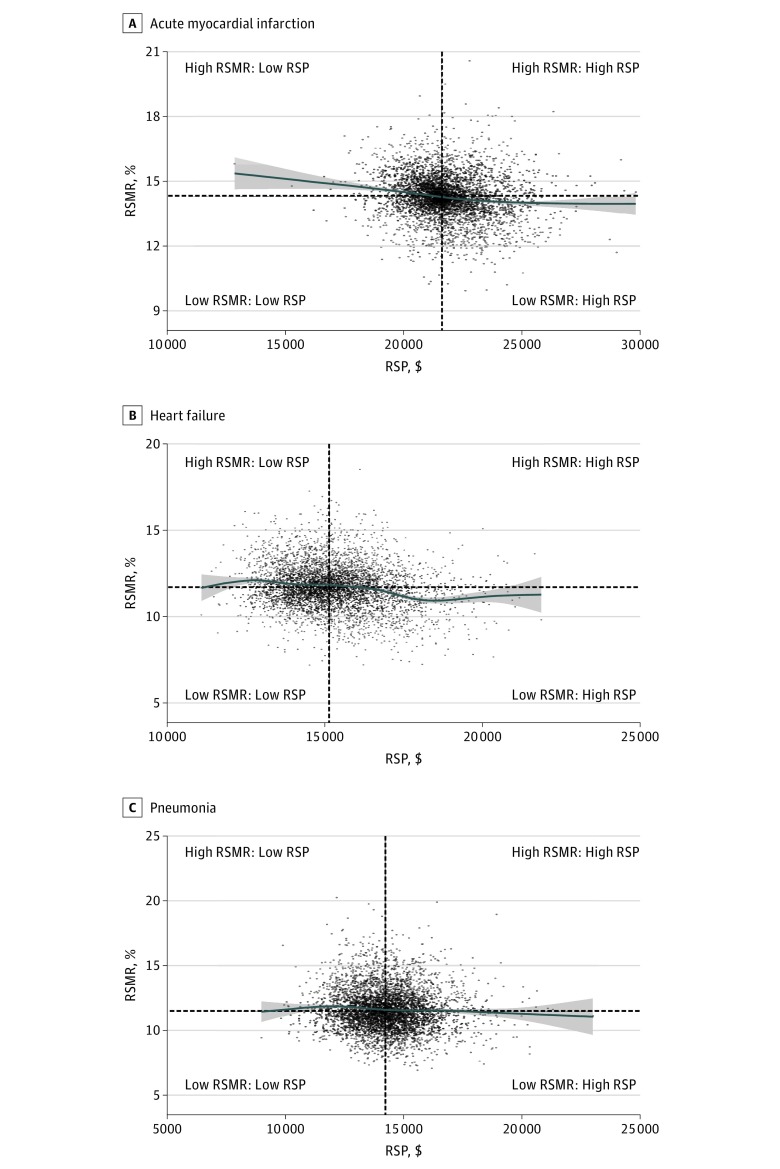
To investigate the association between hospital-level 30-day risk-standardized mortality rates (RSMRs) and 30-day risk-standardized payments (RSPs) for acute myocardial infarction (AMI), heart failure (HF), and pneumonia (PNA); to characterize patterns of value in care; and to identify hospital characteristics associated with high-value care (defined by having lower than median RSMRs and RSPs).
DESIGN, SETTING, AND PARTICIPANTS: This national cross-sectional study applied weighted linear correlation to investigate the association between hospital RSMRs and RSPs for AMI, HF, and PNA between July 1, 2011, and June 30, 2014, among all hospitals; examined correlations in subgroups of hospitals based on key characteristics; and assessed the proportion and characteristics of hospitals delivering high-value care. The data analysis was completed in October 2017. The setting was acute care hospitals. Participants were Medicare fee-for-service beneficiaries discharged with AMI, HF, or PNA.
Hospital-level 30-day RSMRs and RSPs for AMI, HF, and PNA.
The AMI sample consisted of 4339 hospitals with 487 141 hospitalizations for mortality and 462 905 hospitalizations for payment. The HF sample included 4641 hospitals with 960 960 hospitalizations for mortality and 903 721 hospitalizations for payment. The PNA sample contained 4685 hospitals with 952 022 hospitalizations for mortality and 901 764 hospitalizations for payment. The median (interquartile range [IQR]) RSMRs and RSPs, respectively, was 14.3% (IQR, 13.8%-14.8%) and $21 620 (IQR, $20 966-$22 567) for AMI, 11.7% (IQR, 11.0%-12.5%) and $15 139 (IQR, $14 310-$16 118) for HF, and 11.5% (IQR, 10.6%-12.6%) and $14 220 (IQR, $13 342-$15 097) for PNA. There were statistically significant but weak inverse correlations between the RSMRs and RSPs of -0.08 (95% CI, -0.11 to -0.05) for AMI, -0.21 (95% CI, -0.24 to -0.18) for HF, and -0.07 (95% CI, -0.09 to -0.04) for PNA. The largest shared variance between the RSMRs and RSPs was only 4.4% (for HF). The correlations between the RSMRs and RSPs did not differ significantly across teaching status, safety-net status, urban/rural status, or the proportion of patients with low socioeconomic status. Approximately 1 in 4 hospitals (20.9% for AMI, 23.0% for HF, and 23.9% for PNA) had both lower than median RSMRs and RSPs.
These findings suggest that there is significant potential for improvement in the value of AMI, HF, and PNA care and also suggest that high-value care for these conditions is attainable across most hospital types.
支付方和政策制定者一直倡导向基于价值的支付模式转变。然而,人们对医院在护理价值方面的差异程度以及是否存在与高质量护理相关的任何医院特征知之甚少。
调查医院 30 天风险标准化死亡率(RSMR)和 30 天风险标准化支付(RSP)之间的关联,以评估急性心肌梗死(AMI)、心力衰竭(HF)和肺炎(PNA)的护理价值;描述护理价值的模式;并确定与低值 RSMR 和 RSP 相关的高质量护理相关的医院特征(定义为 RSMR 和 RSP 低于中位数)。
设计、设置和参与者:本全国性的横断面研究应用加权线性相关性来研究 2011 年 7 月 1 日至 2014 年 6 月 30 日期间 AMI、HF 和 PNA 所有医院之间的医院 RSMR 和 RSP 之间的关联;根据关键特征对亚组医院的相关性进行了检查;并评估了提供高质量护理的医院的比例和特征。数据分析于 2017 年 10 月完成。该研究地点是急性护理医院。参与者为接受 AMI、HF 或 PNA 治疗出院的医疗保险按服务收费受益人的住院病人。
AMI、HF 和 PNA 的医院 30 天 RSMR 和 RSP。
AMI 样本包括 4339 家医院,共有 487141 例死亡风险和 462905 例支付风险的住院病人。HF 样本包括 4641 家医院,有 960960 例死亡风险和 903721 例支付风险的住院病人。PNA 样本包括 4685 家医院,有 952022 例死亡风险和 901764 例支付风险的住院病人。分别有 14.3%(IQR,13.8%-14.8%)和 21620 美元(IQR,20966-22567 美元)的中位数(四分位距 [IQR])RSMR 和 RSP,HF 分别为 11.7%(IQR,11.0%-12.5%)和 15139 美元(IQR,14310-16118 美元),PNA 分别为 11.5%(IQR,10.6%-12.6%)和 14220 美元(IQR,13342-15097 美元)。AMI 的 RSMR 和 RSP 之间存在统计学上显著但微弱的负相关,分别为-0.08(95%CI,-0.11 至-0.05),HF 为-0.21(95%CI,-0.24 至-0.18),PNA 为-0.07(95%CI,-0.09 至-0.04)。RSMR 和 RSP 之间的最大共享方差仅为 4.4%(HF)。RSMR 和 RSP 之间的相关性在教学状态、安全网状态、城乡状态或低社会经济地位患者比例方面没有显著差异。大约 1/4 的医院(AMI 为 20.9%,HF 为 23.0%,PNA 为 23.9%)的 RSMR 和 RSP 均低于中位数。
这些发现表明,AMI、HF 和 PNA 护理的价值有很大的改进空间,也表明在大多数医院类型中都可以实现这些疾病的高质量护理。