Hoberman Alejandro, Paradise Jack L, Rockette Howard E, Kearney Diana H, Bhatnagar Sonika, Shope Timothy R, Martin Judith M, Kurs-Lasky Marcia, Copelli Susan J, Colborn D Kathleen, Block Stan L, Labella John J, Lynch Thomas G, Cohen Norman L, Haralam MaryAnn, Pope Marcia A, Nagg Jennifer P, Green Michael D, Shaikh Nader
From the Department of Pediatrics, University of Pittsburgh School of Medicine, Children's Hospital of Pittsburgh of the University of Pittsburgh Medical Center (UPMC) (A.H., J.L.P., D.H.K., S.B., T.R.S., J.M.M., M.K.-L., S.J.C., D.K.C., M.H., M.A.P., J.P.N., M.D.G., N.S.), the Department of Biostatistics, Graduate School of Public Health, University of Pittsburgh (H.E.R.), and Children's Community Pediatrics (J.J.L., T.G.L., N.L.C.) - all in Pittsburgh; and Kentucky Pediatric and Adult Research, Bardstown (S.L.B.).
N Engl J Med. 2016 Dec 22;375(25):2446-2456. doi: 10.1056/NEJMoa1606043.
Limiting the duration of antimicrobial treatment constitutes a potential strategy to reduce the risk of antimicrobial resistance among children with acute otitis media.
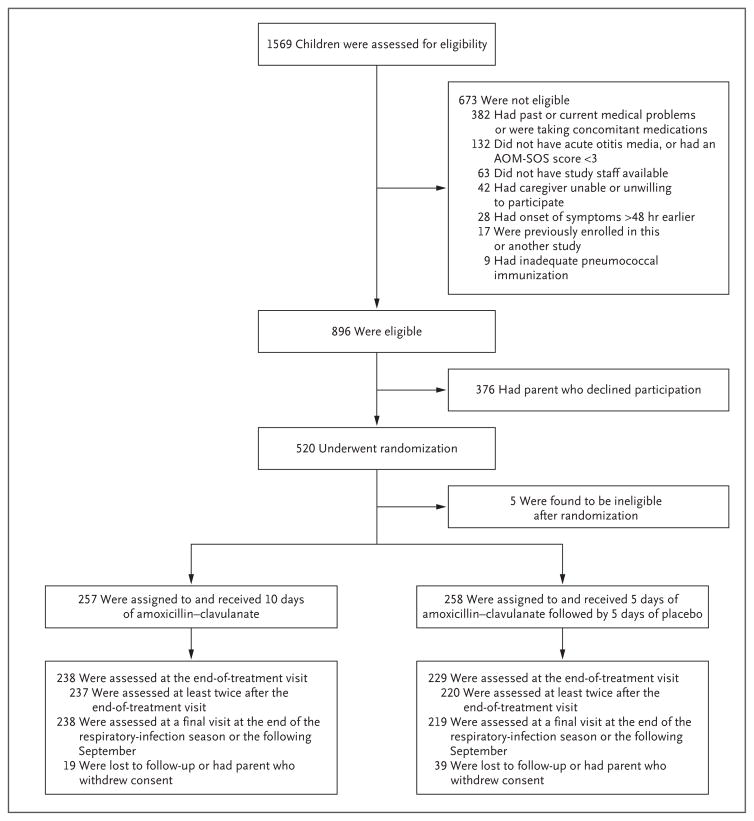
We assigned 520 children, 6 to 23 months of age, with acute otitis media to receive amoxicillin-clavulanate either for a standard duration of 10 days or for a reduced duration of 5 days followed by placebo for 5 days. We measured rates of clinical response (in a systematic fashion, on the basis of signs and symptomatic response), recurrence, and nasopharyngeal colonization, and we analyzed episode outcomes using a noninferiority approach. Symptom scores ranged from 0 to 14, with higher numbers indicating more severe symptoms.
Children who were treated with amoxicillin-clavulanate for 5 days were more likely than those who were treated for 10 days to have clinical failure (77 of 229 children [34%] vs. 39 of 238 [16%]; difference, 17 percentage points [based on unrounded data]; 95% confidence interval, 9 to 25). The mean symptom scores over the period from day 6 to day 14 were 1.61 in the 5-day group and 1.34 in the 10-day group (P=0.07); the mean scores at the day-12-to-14 assessment were 1.89 versus 1.20 (P=0.001). The percentage of children whose symptom scores decreased more than 50% (indicating less severe symptoms) from baseline to the end of treatment was lower in the 5-day group than in the 10-day group (181 of 227 children [80%] vs. 211 of 233 [91%], P=0.003). We found no significant between-group differences in rates of recurrence, adverse events, or nasopharyngeal colonization with penicillin-nonsusceptible pathogens. Clinical-failure rates were greater among children who had been exposed to three or more children for 10 or more hours per week than among those with less exposure (P=0.02) and were also greater among children with infection in both ears than among those with infection in one ear (P<0.001).
Among children 6 to 23 months of age with acute otitis media, reduced-duration antimicrobial treatment resulted in less favorable outcomes than standard-duration treatment; in addition, neither the rate of adverse events nor the rate of emergence of antimicrobial resistance was lower with the shorter regimen. (Funded by the National Institute of Allergy and Infectious Diseases and the National Center for Research Resources; ClinicalTrials.gov number, NCT01511107 .).
限制抗菌治疗的持续时间是降低急性中耳炎患儿抗菌药物耐药风险的一种潜在策略。
我们将520名6至23个月大的急性中耳炎患儿分为两组,一组接受标准疗程10天的阿莫西林 - 克拉维酸治疗,另一组接受缩短疗程5天的阿莫西林 - 克拉维酸治疗,随后5天给予安慰剂。我们以系统的方式测量了临床反应率(基于体征和症状反应)、复发率和鼻咽部定植情况,并采用非劣效性方法分析了各病例的结局。症状评分范围为0至14分,分数越高表明症状越严重。
接受5天阿莫西林 - 克拉维酸治疗的患儿比接受10天治疗的患儿更易出现临床治疗失败(229名患儿中有77名[34%],而238名中有39名[16%];差异为17个百分点[基于未四舍五入的数据];95%置信区间为9至25)。在第6天至第14天期间,5天治疗组的平均症状评分为1.61,10天治疗组为1.34(P = 0.07);在第12天至第14天评估时,平均评分分别为1.89和1.20(P = 0.001)。从基线到治疗结束症状评分下降超过50%(表明症状减轻)的患儿百分比,5天治疗组低于10天治疗组(227名患儿中有181名[80%],而233名中有211名[91%],P = 0.003)。我们发现两组在复发率、不良事件发生率或对青霉素不敏感病原体的鼻咽部定植率方面无显著差异。每周接触三个或更多儿童达10小时或更长时间的患儿临床治疗失败率高于接触较少的患儿(P = 0.02),双耳感染患儿的临床治疗失败率也高于单耳感染患儿(P < 0.001)。
在6至23个月大的急性中耳炎患儿中,缩短疗程的抗菌治疗效果不如标准疗程治疗;此外,较短疗程治疗的不良事件发生率和抗菌药物耐药发生率均未降低。(由美国国立过敏与传染病研究所和国家研究资源中心资助;ClinicalTrials.gov编号,NCT01511107。)