Henao-Restrepo Ana Maria, Camacho Anton, Longini Ira M, Watson Conall H, Edmunds W John, Egger Matthias, Carroll Miles W, Dean Natalie E, Diatta Ibrahima, Doumbia Moussa, Draguez Bertrand, Duraffour Sophie, Enwere Godwin, Grais Rebecca, Gunther Stephan, Gsell Pierre-Stéphane, Hossmann Stefanie, Watle Sara Viksmoen, Kondé Mandy Kader, Kéïta Sakoba, Kone Souleymane, Kuisma Eewa, Levine Myron M, Mandal Sema, Mauget Thomas, Norheim Gunnstein, Riveros Ximena, Soumah Aboubacar, Trelle Sven, Vicari Andrea S, Røttingen John-Arne, Kieny Marie-Paule
WHO, Geneva, Switzerland.
Faculty of Epidemiology and Population Health, London School of Hygiene & Tropical Medicine, London, UK.
Lancet. 2017 Feb 4;389(10068):505-518. doi: 10.1016/S0140-6736(16)32621-6. Epub 2016 Dec 23.
rVSV-ZEBOV is a recombinant, replication competent vesicular stomatitis virus-based candidate vaccine expressing a surface glycoprotein of Zaire Ebolavirus. We tested the effect of rVSV-ZEBOV in preventing Ebola virus disease in contacts and contacts of contacts of recently confirmed cases in Guinea, west Africa.
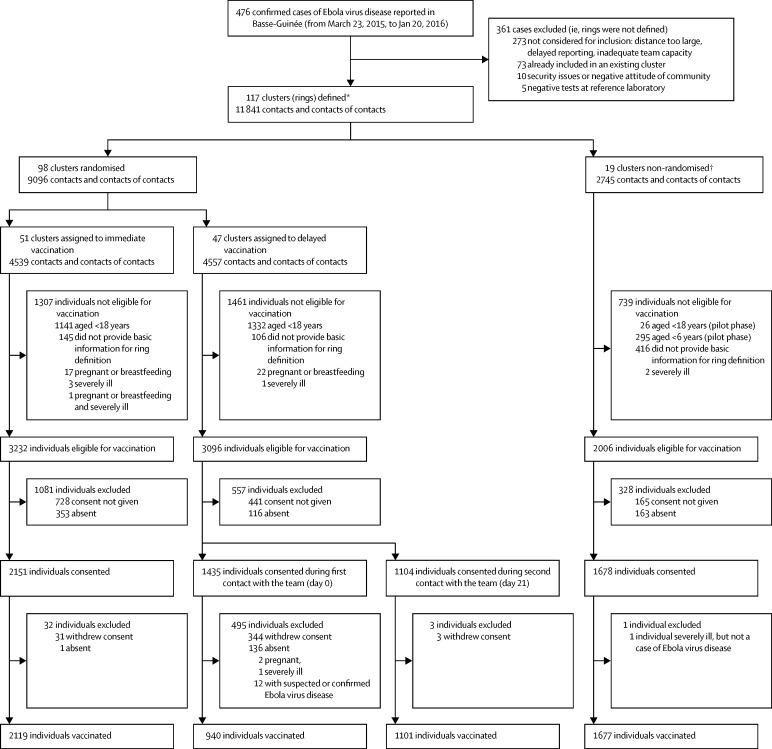
We did an open-label, cluster-randomised ring vaccination trial (Ebola ça Suffit!) in the communities of Conakry and eight surrounding prefectures in the Basse-Guinée region of Guinea, and in Tomkolili and Bombali in Sierra Leone. We assessed the efficacy of a single intramuscular dose of rVSV-ZEBOV (2×10 plaque-forming units administered in the deltoid muscle) in the prevention of laboratory confirmed Ebola virus disease. After confirmation of a case of Ebola virus disease, we definitively enumerated on a list a ring (cluster) of all their contacts and contacts of contacts including named contacts and contacts of contacts who were absent at the time of the trial team visit. The list was archived, then we randomly assigned clusters (1:1) to either immediate vaccination or delayed vaccination (21 days later) of all eligible individuals (eg, those aged ≥18 years and not pregnant, breastfeeding, or severely ill). An independent statistician generated the assignment sequence using block randomisation with randomly varying blocks, stratified by location (urban vs rural) and size of rings (≤20 individuals vs >20 individuals). Ebola response teams and laboratory workers were unaware of assignments. After a recommendation by an independent data and safety monitoring board, randomisation was stopped and immediate vaccination was also offered to children aged 6-17 years and all identified rings. The prespecified primary outcome was a laboratory confirmed case of Ebola virus disease with onset 10 days or more from randomisation. The primary analysis compared the incidence of Ebola virus disease in eligible and vaccinated individuals assigned to immediate vaccination versus eligible contacts and contacts of contacts assigned to delayed vaccination. This trial is registered with the Pan African Clinical Trials Registry, number PACTR201503001057193.
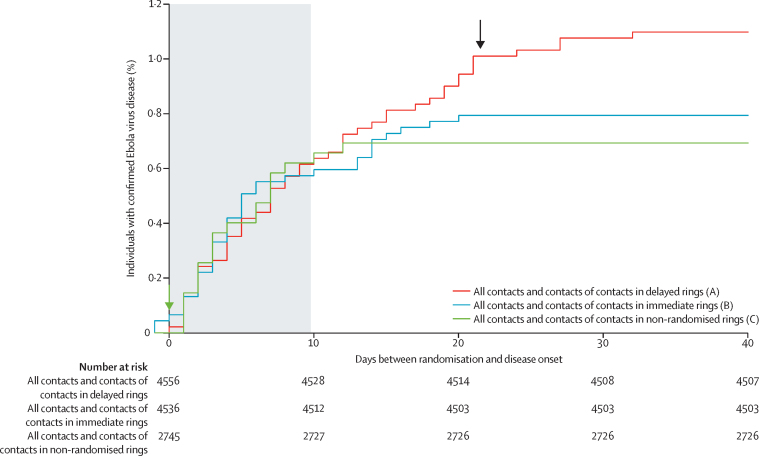
In the randomised part of the trial we identified 4539 contacts and contacts of contacts in 51 clusters randomly assigned to immediate vaccination (of whom 3232 were eligible, 2151 consented, and 2119 were immediately vaccinated) and 4557 contacts and contacts of contacts in 47 clusters randomly assigned to delayed vaccination (of whom 3096 were eligible, 2539 consented, and 2041 were vaccinated 21 days after randomisation). No cases of Ebola virus disease occurred 10 days or more after randomisation among randomly assigned contacts and contacts of contacts vaccinated in immediate clusters versus 16 cases (7 clusters affected) among all eligible individuals in delayed clusters. Vaccine efficacy was 100% (95% CI 68·9-100·0, p=0·0045), and the calculated intraclass correlation coefficient was 0·035. Additionally, we defined 19 non-randomised clusters in which we enumerated 2745 contacts and contacts of contacts, 2006 of whom were eligible and 1677 were immediately vaccinated, including 194 children. The evidence from all 117 clusters showed that no cases of Ebola virus disease occurred 10 days or more after randomisation among all immediately vaccinated contacts and contacts of contacts versus 23 cases (11 clusters affected) among all eligible contacts and contacts of contacts in delayed plus all eligible contacts and contacts of contacts never vaccinated in immediate clusters. The estimated vaccine efficacy here was 100% (95% CI 79·3-100·0, p=0·0033). 52% of contacts and contacts of contacts assigned to immediate vaccination and in non-randomised clusters received the vaccine immediately; vaccination protected both vaccinated and unvaccinated people in those clusters. 5837 individuals in total received the vaccine (5643 adults and 194 children), and all vaccinees were followed up for 84 days. 3149 (53·9%) of 5837 individuals reported at least one adverse event in the 14 days after vaccination; these were typically mild (87·5% of all 7211 adverse events). Headache (1832 [25·4%]), fatigue (1361 [18·9%]), and muscle pain (942 [13·1%]) were the most commonly reported adverse events in this period across all age groups. 80 serious adverse events were identified, of which two were judged to be related to vaccination (one febrile reaction and one anaphylaxis) and one possibly related (influenza-like illness); all three recovered without sequelae.
The results add weight to the interim assessment that rVSV-ZEBOV offers substantial protection against Ebola virus disease, with no cases among vaccinated individuals from day 10 after vaccination in both randomised and non-randomised clusters.
WHO, UK Wellcome Trust, the UK Government through the Department of International Development, Médecins Sans Frontières, Norwegian Ministry of Foreign Affairs (through the Research Council of Norway's GLOBVAC programme), and the Canadian Government (through the Public Health Agency of Canada, Canadian Institutes of Health Research, International Development Research Centre and Department of Foreign Affairs, Trade and Development).
rVSV-ZEBOV是一种重组的、具有复制能力的基于水疱性口炎病毒的候选疫苗,表达扎伊尔埃博拉病毒的表面糖蛋白。我们在西非几内亚最近确诊病例的接触者以及接触者的接触者中测试了rVSV-ZEBOV预防埃博拉病毒病的效果。
我们在几内亚下几内亚地区科纳克里市及周边八个行政区的社区,以及塞拉利昂的通科利利和邦巴利开展了一项开放标签、整群随机环式疫苗接种试验(埃博拉到此为止!)。我们评估了单剂肌内注射rVSV-ZEBOV(2×10空斑形成单位,注射于三角肌)预防实验室确诊的埃博拉病毒病的效力。确诊埃博拉病毒病病例后,我们在一份名单上明确列出其所有接触者以及接触者的接触者组成的环(群组),包括在试验团队访视时不在场的指名接触者和接触者的接触者。该名单存档后,我们将群组(1:1)随机分配给所有符合条件的个体(如年龄≥18岁、未怀孕、未哺乳或未患重病者)立即接种疫苗或延迟接种疫苗(21天后)。一名独立统计学家使用随机分块随机化方法生成分配序列,随机分块大小可变,按地点(城市与农村)和环的大小(≤20人对>20人)分层。埃博拉应对小组和实验室工作人员不知道分配情况。经独立数据与安全监测委员会建议,随机化停止,6-17岁儿童和所有已识别的环也被提供立即接种疫苗。预先设定的主要结局是随机分组后10天或更长时间出现的实验室确诊的埃博拉病毒病病例。主要分析比较了分配到立即接种疫苗的符合条件且接种疫苗的个体与分配到延迟接种疫苗的符合条件的接触者以及接触者的接触者中埃博拉病毒病的发病率。本试验已在泛非临床试验注册中心注册,注册号为PACTR201503001057193。
在试验的随机分组部分,我们在随机分配到立即接种疫苗的51个群组中识别出4539名接触者以及接触者的接触者(其中3232名符合条件,2151名同意接种,2119名立即接种),在随机分配到延迟接种疫苗的47个群组中识别出4557名接触者以及接触者的接触者(其中3096名符合条件,2539名同意接种,2041名在随机分组后21天接种)。在立即接种疫苗的群组中随机分配的接触者以及接触者的接触者中,随机分组后10天或更长时间未出现埃博拉病毒病病例,而在延迟接种疫苗的群组中所有符合条件的个体中有16例(涉及7个群组)发病。疫苗效力为100%(95%CI 68·9-100·0,p=0·0045),计算得到的组内相关系数为0·035。此外,我们定义了19个非随机分组的群组,在其中我们列出了2745名接触者以及接触者的接触者,其中2006名符合条件,1677名立即接种了疫苗,包括194名儿童。来自所有117个群组的证据显示,在所有立即接种疫苗的接触者以及接触者的接触者中,随机分组后10天或更长时间未出现埃博拉病毒病病例,而在延迟接种疫苗的所有符合条件的接触者以及接触者加上立即接种疫苗的群组中从未接种疫苗的所有符合条件的接触者以及接触者中有23例(涉及11个群组)发病。此处估计的疫苗效力为100%(95%CI 79·3-100·0,p=0·0033)。分配到立即接种疫苗的接触者以及接触者中,52%在立即接种疫苗的群组和非随机分组的群组中立即接种了疫苗;接种疫苗保护了这些群组中已接种和未接种疫苗的人群。共有5837人接种了疫苗(5643名成人和194名儿童),所有疫苗接种者均随访了84天。5837名个体中有3