Artenstein Andrew W, Friderici Jennifer, Holers Adam, Lewis Deirdre, Fitzgerald Jan, Visintainer Paul
Department of Medicine, Baystate Health; University of Massachusetts Medical School-Baystate.
Academic Affairs, Baystate Health , Springfield, Massachusetts.
Open Forum Infect Dis. 2016 Sep 14;3(4):ofw191. doi: 10.1093/ofid/ofw191. eCollection 2016 Oct.
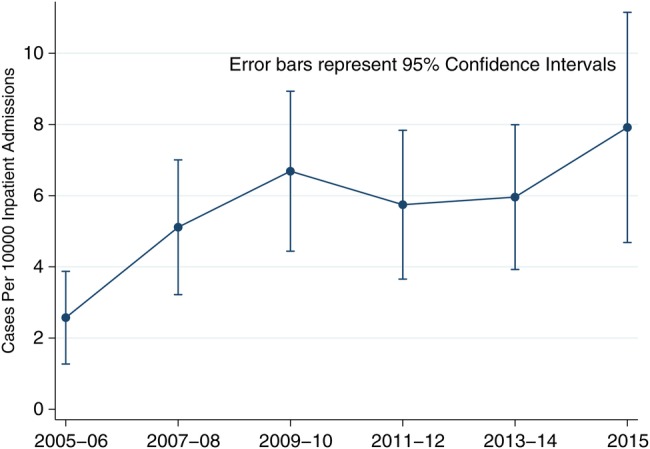
Delayed recognition of spinal epidural abscess (SEA) contributes to poor outcomes from this highly morbid and potentially lethal infection. We performed a case-control study in a regional, high-volume, tertiary care, academic medical center over the years 2005-2015 to assess the potential changing epidemiology, clinical and laboratory manifestations, and course of this disorder and to identify factors that might lead to early identification of SEA. Diagnostic billing codes consistent with SEA were used to identify inpatient admissions for abstraction. Subjects were categorized as cases or controls based on the results of spinal imaging studies. Characteristics were compared using Fisher's exact or Kruskal-Wallis tests. All values were 2-sided with a critical threshold of <.05. We identified 162 cases and 88 controls during the study period. The incidence of SEA increased from 2.5 to 8.0 per 10 000 admissions, a 3.3-fold change from 2005 to 2015 ( < .001 for the linear trend). Compared with controls, cases were significantly more likely to have experienced at least 1 previous healthcare visit or received antimicrobials within 30 days of admission; to have comorbidities of injection drug use, alcohol abuse, or obesity; and to manifest fever or rigors. Cases were also more likely to harbor coinfection at a noncontiguous site. When available, inflammatory markers were noted to be markedly elevated in cases. Focal neurologic deficits were seen with similar frequencies in both groups. Based on our analysis, it appears that selected factors noted at the time of clinical presentation may facilitate early recognition of SEA.
脊柱硬膜外脓肿(SEA)的延迟诊断会导致这种高发病率且可能致命的感染产生不良后果。我们于2005年至2015年期间在一家地区性、高容量、三级医疗学术医学中心开展了一项病例对照研究,以评估该疾病潜在的流行病学变化、临床和实验室表现及病程,并确定可能有助于早期识别SEA的因素。使用与SEA一致的诊断计费代码来识别需提取信息的住院患者。根据脊柱影像学研究结果将受试者分为病例组或对照组。使用Fisher精确检验或Kruskal-Wallis检验比较特征。所有P值均为双侧,临界阈值为<0.05。在研究期间,我们共识别出162例病例和88例对照。SEA的发病率从每10000例入院患者中的2.5例增至8.0例,2005年至2015年变化了3.3倍(线性趋势P<0.001)。与对照组相比,病例组更有可能在入院前至少有过1次医疗就诊或在入院30天内接受过抗菌药物治疗;更有可能有注射吸毒、酗酒或肥胖等合并症;更有可能出现发热或寒战。病例组也更有可能在非相邻部位合并感染。在有炎症标志物数据时,病例组的炎症标志物明显升高。两组出现局灶性神经功能缺损的频率相似。基于我们的分析,似乎在临床表现时所注意到的某些因素可能有助于早期识别SEA。