Hooli Shubhada, Colbourn Tim, Lufesi Norman, Costello Anthony, Nambiar Bejoy, Thammasitboon Satid, Makwenda Charles, Mwansambo Charles, McCollum Eric D, King Carina
Department of Pediatrics, Section of Critical Care Medicine, Baylor College of Medicine and Texas Children's Hospital, Houston, United States of America.
Department of Pediatrics, Section of Emergency Medicine, Baylor College of Medicine and Texas Children's Hospital, Houston, United States of America.
PLoS One. 2016 Dec 28;11(12):e0168126. doi: 10.1371/journal.pone.0168126. eCollection 2016.
Pneumonia is the leading infectious cause of under-5 mortality in sub-Saharan Africa. Clinical prediction tools may aide case classification, triage, and allocation of hospital resources. We performed an external validation of two published prediction tools and compared this to a locally developed tool to identify children admitted with pneumonia at increased risk for in-hospital mortality in Malawi.
We retrospectively analyzed the performance of the Respiratory Index of Severity in Children (RISC) and modified RISC (mRISC) scores in a child pneumonia dataset prospectively collected during routine care at seven hospitals in Malawi between 2011-2014. RISC has both an HIV-infected and HIV-uninfected tool. A local score (RISC-Malawi) was developed using multivariable logistic regression with missing data multiply imputed using chained equations. Score performances were assessed using c-statistics, sensitivity, specificity, positive predictive value, negative predictive value, and likelihood statistics.
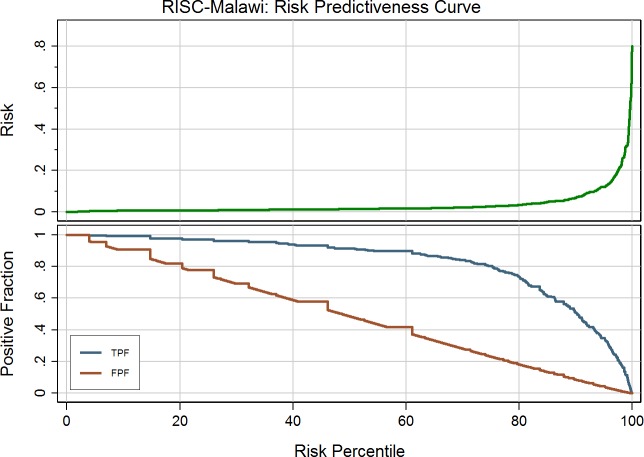
16,475 in-patient pneumonia episodes were recorded (case-fatality rate (CFR): 3.2%), 9,533 with complete data (CFR: 2.0%). The c-statistic for the RISC (HIV-uninfected) score, used to assess its ability to differentiate between children who survived to discharge and those that died, was 0.72. The RISC-Malawi score, using mid-upper arm circumference as an indicator of malnutrition severity, had a c-statistic of 0.79. We were unable to perform a comprehensive external validation of RISC (HIV-infected) and mRISC as both scores include parameters that were not routinely documented variables in our dataset.
In our population of Malawian children with WHO-defined pneumonia, the RISC (HIV-uninfected) score identified those at high risk for in-hospital mortality. However the refinement of parameters and resultant creation of RISC-Malawi improved performance. Next steps include prospectively studying both scores to determine if incorporation into routine care delivery can have a meaningful impact on in-hospital CFRs of children with WHO-defined pneumonia.
肺炎是撒哈拉以南非洲5岁以下儿童死亡的主要感染原因。临床预测工具可能有助于病例分类、分诊和医院资源分配。我们对两种已发表的预测工具进行了外部验证,并将其与本地开发的工具进行比较,以识别马拉维因肺炎入院且院内死亡风险增加的儿童。
我们回顾性分析了2011年至2014年期间在马拉维七家医院常规护理期间前瞻性收集的儿童肺炎数据集中儿童呼吸严重程度指数(RISC)和改良RISC(mRISC)评分的表现。RISC有针对HIV感染儿童和未感染儿童的工具。使用多变量逻辑回归开发了一个本地评分(RISC-马拉维),使用链式方程对缺失数据进行多重插补。使用c统计量、敏感性、特异性、阳性预测值、阴性预测值和似然统计量评估评分表现。
记录了16475例住院肺炎病例(病死率(CFR):3.2%),9533例有完整数据(CFR:2.0%)。用于评估其区分存活至出院儿童和死亡儿童能力的RISC(未感染HIV)评分的c统计量为0.72。以中上臂围作为营养不良严重程度指标的RISC-马拉维评分的c统计量为0.79。我们无法对RISC(感染HIV)和mRISC进行全面的外部验证,因为这两个评分都包含我们数据集中未常规记录的变量参数。
在我们患有世界卫生组织定义的肺炎的马拉维儿童人群中,RISC(未感染HIV)评分识别出了院内死亡风险高的儿童。然而,参数的细化以及由此产生的RISC-马拉维评分提高了性能。下一步包括对这两个评分进行前瞻性研究,以确定将其纳入常规护理是否会对患有世界卫生组织定义的肺炎的儿童的院内CFR产生有意义的影响。