Division of Pediatric Emergency Medicine, Emory University School of Medicine, Children's Healthcare of Atlanta, Atlanta, Georgia, USA.
Section of Pediatric Emergency Medicine, Texas Children's Hospital, Baylor College of Medicine, Houston, Texas, USA.
J Glob Health. 2021 Oct 9;11:04062. doi: 10.7189/jogh.11.04062. eCollection 2021.
Existing scores to identify children at risk of hospitalized pneumonia-related mortality lack broad external validation. Our objective was to externally validate three such risk scores.
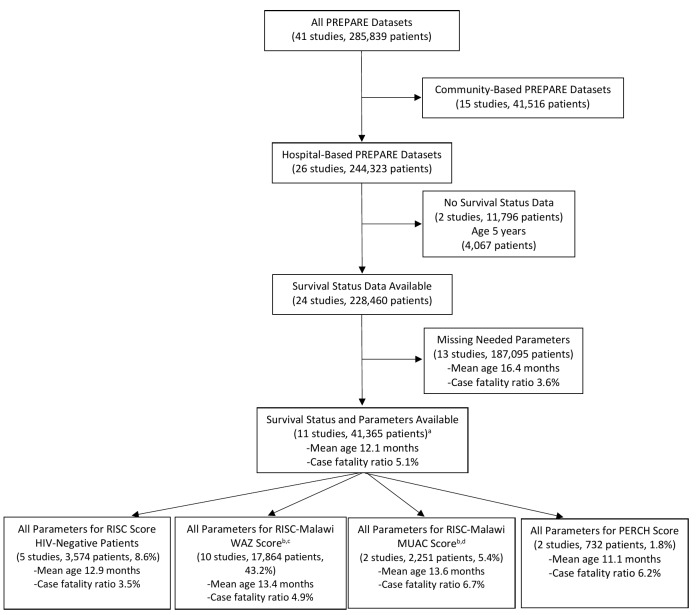
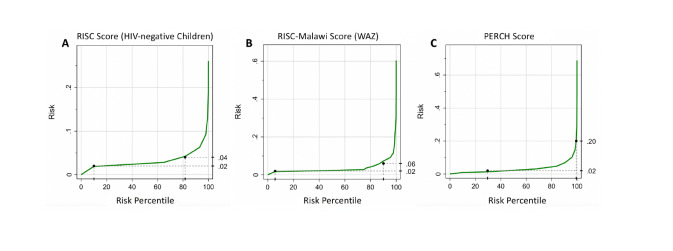
We applied the Respiratory Index of Severity in Children (RISC) for HIV-negative children, the RISC-Malawi, and the Pneumonia Etiology Research for Child Health (PERCH) scores to hospitalized children in the Pneumonia REsearch Partnerships to Assess WHO REcommendations (PREPARE) data set. The PREPARE data set includes pooled data from 41 studies on pediatric pneumonia from across the world. We calculated test characteristics and the area under the curve (AUC) for each of these clinical prediction rules.
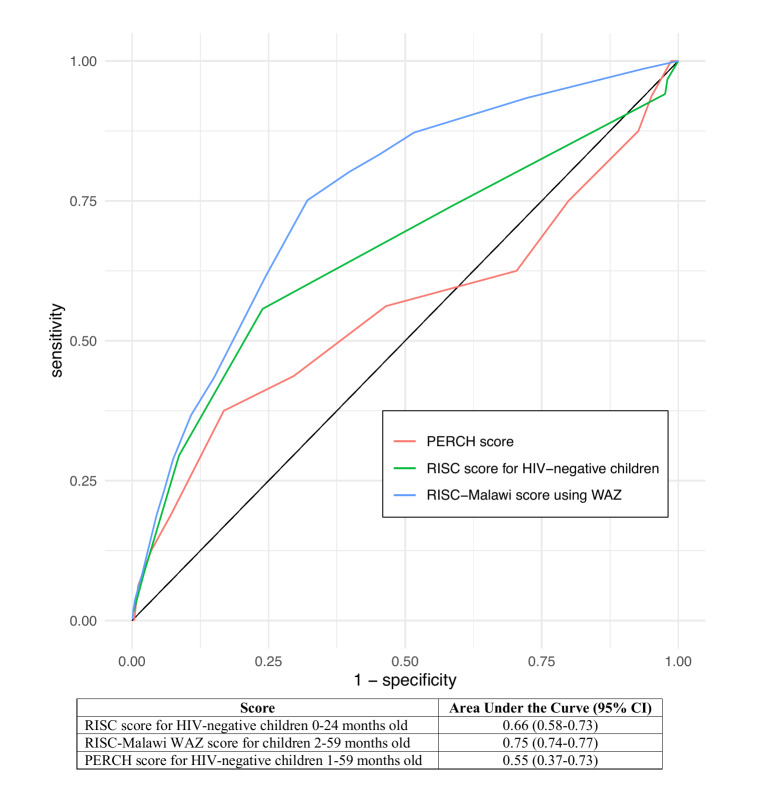
The RISC score for HIV-negative children was applied to 3574 children 0-24 months and demonstrated poor discriminatory ability (AUC = 0.66, 95% confidence interval (CI) = 0.58-0.73) in the identification of children at risk of hospitalized pneumonia-related mortality. The RISC-Malawi score had fair discriminatory value (AUC = 0.75, 95% CI = 0.74-0.77) among 17 864 children 2-59 months. The PERCH score was applied to 732 children 1-59 months and also demonstrated poor discriminatory value (AUC = 0.55, 95% CI = 0.37-0.73).
In a large external application of the RISC, RISC-Malawi, and PERCH scores, a substantial number of children were misclassified for their risk of hospitalized pneumonia-related mortality. Although pneumonia risk scores have performed well among the cohorts in which they were derived, their performance diminished when externally applied. A generalizable risk assessment tool with higher sensitivity and specificity to identify children at risk of hospitalized pneumonia-related mortality may be needed. Such a generalizable risk assessment tool would need context-specific validation prior to implementation in that setting.
现有的识别与住院肺炎相关死亡风险的儿童的评分系统缺乏广泛的外部验证。我们的目标是对三种这样的风险评分系统进行外部验证。
我们将儿童呼吸危重症指数(RISC)评分系统、RISC-马拉维评分系统和肺炎病因研究以评估儿童健康的世卫组织推荐(PERCH)评分系统应用于全球范围内 41 项儿科肺炎研究的肺炎研究伙伴关系以评估世卫组织建议(PREPARE)数据集的住院儿童中。PREPARE 数据集包括来自世界各地的儿科肺炎研究的汇总数据。我们计算了这些临床预测规则的各项测试特征和曲线下面积(AUC)。
适用于 3574 名 0-24 个月的 HIV 阴性儿童的 RISC 评分系统在识别与住院肺炎相关死亡风险的儿童方面表现出较差的区分能力(AUC=0.66,95%置信区间[CI]:0.58-0.73)。适用于 17864 名 2-59 个月儿童的 RISC-马拉维评分系统具有较好的区分能力(AUC=0.75,95%CI:0.74-0.77)。PERCH 评分系统适用于 732 名 1-59 个月的儿童,其区分能力也较差(AUC=0.55,95%CI:0.37-0.73)。
在 RISC、RISC-马拉维评分系统和 PERCH 评分系统的大规模外部应用中,大量儿童的住院肺炎相关死亡风险被错误分类。尽管肺炎风险评分系统在其衍生的队列中表现良好,但在外部应用时,其性能会下降。可能需要一种具有更高敏感性和特异性的可推广风险评估工具,以识别与住院肺炎相关死亡风险的儿童。在该环境中实施之前,这种可推广的风险评估工具需要进行特定于上下文的验证。