Ekerstad Niklas, Karlson Björn W, Dahlin Ivanoff Synneve, Landahl Sten, Andersson David, Heintz Emelie, Husberg Magnus, Alwin Jenny
Department of Cardiology, NU (NÄL-Uddevalla) Hospital Group, Trollhattan; Division of Health Care Analysis, Department of Medical and Health Sciences, Linköping University, Linköping.
Department of Molecular and Clinical Medicine, Institute of Medicine.
Clin Interv Aging. 2016 Dec 16;12:1-9. doi: 10.2147/CIA.S124003. eCollection 2017.
The aim of this study was to investigate whether the acute care of frail elderly patients in a comprehensive geriatric assessment (CGA) unit is superior to the care in a conventional acute medical care unit.
This is a clinical, prospective, randomized, controlled, one-center intervention study.
This study was conducted in a large county hospital in western Sweden.
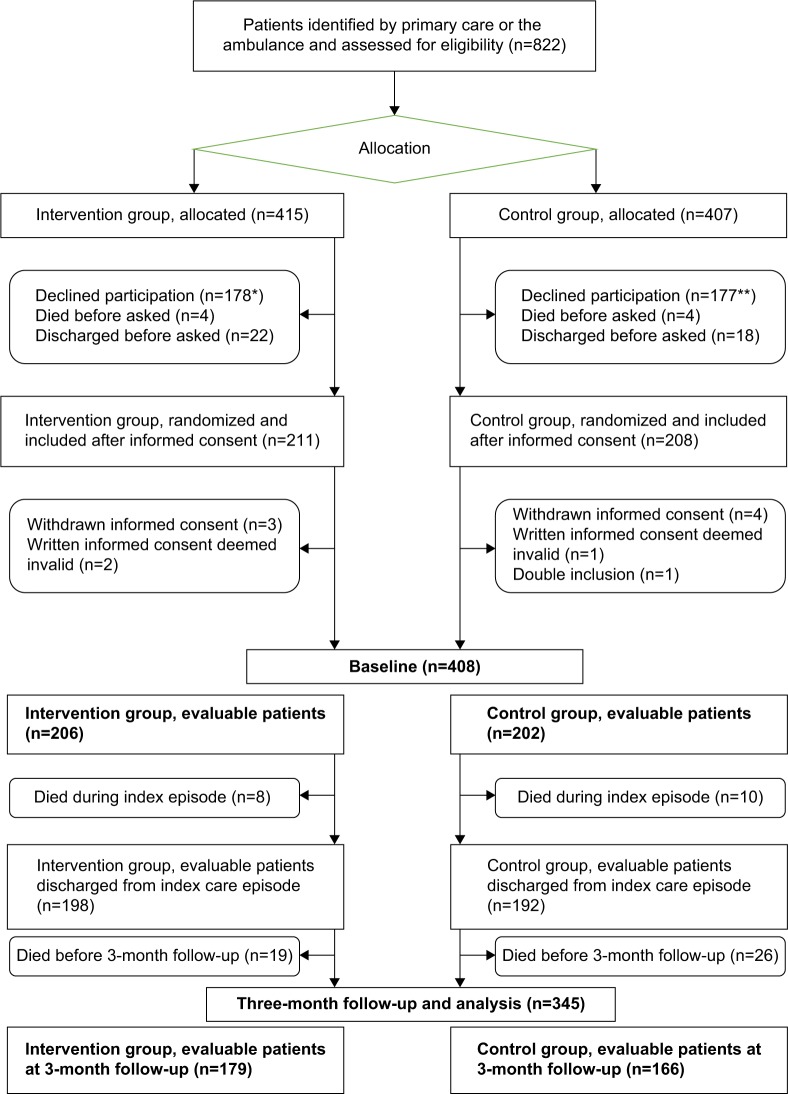
The study included 408 frail elderly patients, aged ≥75 years, in need of acute in-hospital treatment. The patients were allocated to the intervention group (n=206) or control group (n=202). Mean age of the patients was 85.7 years, and 56% were female.
This organizational form of care is characterized by a structured, systematic interdisciplinary CGA-based care at an acute elderly care unit.
The primary outcome was the change in health-related quality of life (HRQoL) 3 months after discharge from hospital, measured by the Health Utilities Index-3 (HUI-3). Secondary outcomes were all-cause mortality, rehospitalizations, and hospital care costs.
After adjustment by regression analysis, patients in the intervention group were less likely to present with decline in HRQoL after 3 months for the following dimensions: vision (odds ratio [OR] =0.33, 95% confidence interval [CI] =0.14-0.79), ambulation (OR =0.19, 95% CI =0.1-0.37), dexterity (OR =0.38, 95% CI =0.19-0.75), emotion (OR =0.43, 95% CI =0.22-0.84), cognition (OR = 0.076, 95% CI =0.033-0.18) and pain (OR =0.28, 95% CI =0.15-0.50). Treatment in a CGA unit was independently associated with lower 3-month mortality adjusted by Cox regression analysis (hazard ratio [HR] =0.55, 95% CI =0.32-0.96), and the two groups did not differ significantly in terms of hospital care costs (>0.05).
Patients in an acute CGA unit were less likely to present with decline in HRQoL after 3 months, and the care in a CGA unit was also independently associated with lower mortality, at no higher cost.
本研究旨在调查在综合老年评估(CGA)病房对体弱老年患者进行的急性护理是否优于传统急性医疗病房的护理。
这是一项临床、前瞻性、随机、对照、单中心干预研究。
本研究在瑞典西部的一家大型县医院进行。
该研究纳入了408名年龄≥75岁、需要住院急性治疗的体弱老年患者。这些患者被分配到干预组(n = 206)或对照组(n = 202)。患者的平均年龄为85.7岁,56%为女性。
这种护理组织形式的特点是在急性老年护理病房基于结构化、系统性的跨学科CGA进行护理。
主要结局是出院3个月后用健康效用指数-3(HUI-3)测量的健康相关生活质量(HRQoL)的变化。次要结局是全因死亡率、再入院率和医院护理费用。
经回归分析调整后,干预组患者在3个月后以下维度的HRQoL下降的可能性较小:视力(比值比[OR]=0.33,95%置信区间[CI]=0.14 - 0.79)、行走能力(OR = 0.19,95% CI = 0.1 - 0.37)、灵活性(OR = 0.38,95% CI = 0.19 - 0.75)、情绪(OR = 0.43,95% CI = 0.22 - 0.84)、认知(OR = 0.076,95% CI = 0.033 - 0.18)和疼痛(OR = 0.28,95% CI = 0.15 - 0.50)。经Cox回归分析调整后,在CGA病房接受治疗与较低的3个月死亡率独立相关(风险比[HR]=0.55,95% CI = 0.32 - 0.96),且两组在医院护理费用方面无显著差异(>0.05)。
急性CGA病房的患者在3个月后HRQoL下降的可能性较小,且CGA病房的护理也与较低的死亡率独立相关,同时成本不更高。