Shen Jun-Yi, Li Chuan, Wen Tian-Fu, Yan Lv-Nan, Li Bo, Wang Wen-Tao, Yang Jia-Yin, Xu Ming-Qing, Nazar Highness Tholakkara
Department of Liver Surgery & Liver Transplantation Center, West China Hospital, Sichuan University, Chengdu, China.
Medicine (Baltimore). 2016 Dec;95(52):e5756. doi: 10.1097/MD.0000000000005756.
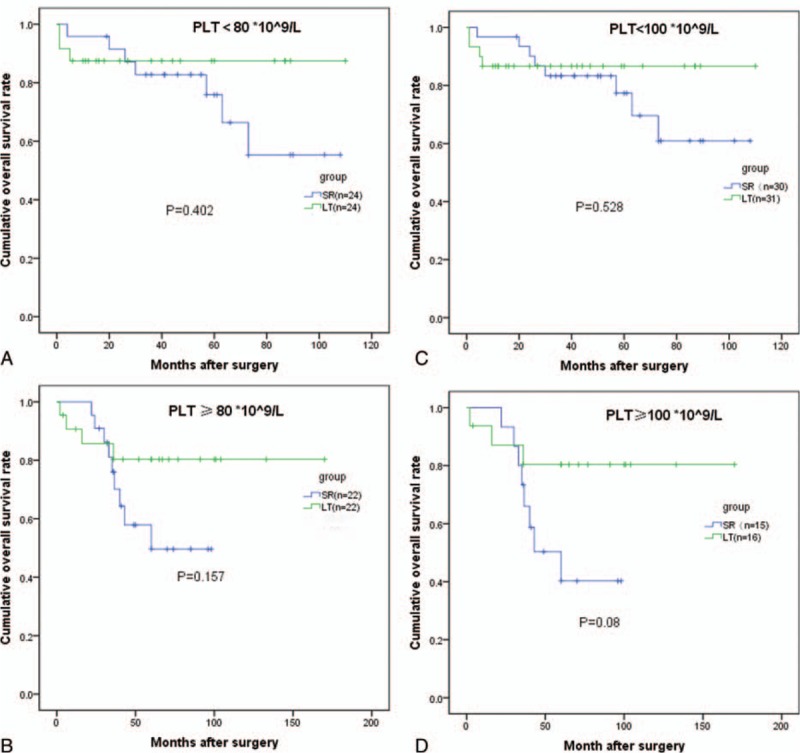
The optimal treatment (liver transplantation [LT] vs surgical resection [SR]) for early-stage hepatocellular carcinoma (HCC) remains controversial.A total of 209 SR patients and 129 LT patients were identified at our institution. After eliminating 27 patients with Child-Pugh C, the data from 209 SR patients and 102 LT patients were analyzed using a propensity score matching (PSM) model. Forty-six pairs were generated. A subgroup analysis was conducted based on the alpha-fetoprotein (AFP) level or platelet count (PLT). A survival analysis was performed using the Kaplan-Meier method.Gender, satellite lesions, and the treatment method were predictors of HCC recurrence. The Ishak score and treatment methods were associated with long-term survival after surgery. Before PSM, LT patients had a better prognosis than those treated by SR. Among HCC patients with childhood A/B cirrhosis, after PSM, SR achieved similar overall survival outcomes compared with LT. LT and SR resulted in comparable long-term survival for patients with or without thrombocytopenia. Patients with an AFP ≥ 400 ng/mL might achieve more survival benefits from LT.Our propensity score model provided evidence that, compared with transplantation, surgical resection could result in comparable long-term survival for resectable early-stage HCC patients, except for the AFP ≥ 400 ng/mL HCC subgroup. Surgical resection might not be a contraindication for early-stage HCC patients with thrombocytopenia due to their similar prognosis after transplantation.
早期肝细胞癌(HCC)的最佳治疗方法(肝移植[LT]与手术切除[SR])仍存在争议。我们机构共确定了209例接受手术切除的患者和129例接受肝移植的患者。在排除27例Child-Pugh C级患者后,使用倾向评分匹配(PSM)模型对209例手术切除患者和102例肝移植患者的数据进行了分析。生成了46对匹配数据。根据甲胎蛋白(AFP)水平或血小板计数(PLT)进行了亚组分析。采用Kaplan-Meier法进行生存分析。性别、卫星灶和治疗方法是HCC复发的预测因素。Ishak评分和治疗方法与术后长期生存相关。在进行倾向评分匹配之前,肝移植患者的预后优于接受手术切除的患者。在患有Child-Pugh A/B级肝硬化的HCC患者中,倾向评分匹配后,手术切除与肝移植的总生存结果相似。肝移植和手术切除在血小板减少和非血小板减少患者中产生了相当的长期生存率。AFP≥400 ng/mL的患者可能从肝移植中获得更多生存益处。我们的倾向评分模型提供了证据,表明与移植相比,手术切除对于可切除的早期HCC患者可产生相当的长期生存率,但AFP≥400 ng/mL的HCC亚组除外。由于血小板减少的早期HCC患者移植后的预后相似,手术切除可能不是其禁忌证。