van den Brand Jan A J G, Mutsaers Henricus A M, van Zuilen Arjan D, Blankestijn Peter J, van den Broek Petra H, Russel Frans G M, Masereeuw Rosalinde, Wetzels Jack F M
Department of Nephrology, Radboud Institute of Health Sciences, Radboud University Medical Center, Nijmegen, The Netherlands.
Department of Pharmaceutical Technology and Biopharmacy, University of Groningen, Groningen, The Netherlands.
PLoS One. 2016 Dec 29;11(12):e0168117. doi: 10.1371/journal.pone.0168117. eCollection 2016.
To date, over 150 possible uremic solutes have been listed, but their role in the progression of CKD is largely unknown. Here, the association between a selected panel of uremic solutes and progression in CKD patients was investigated.
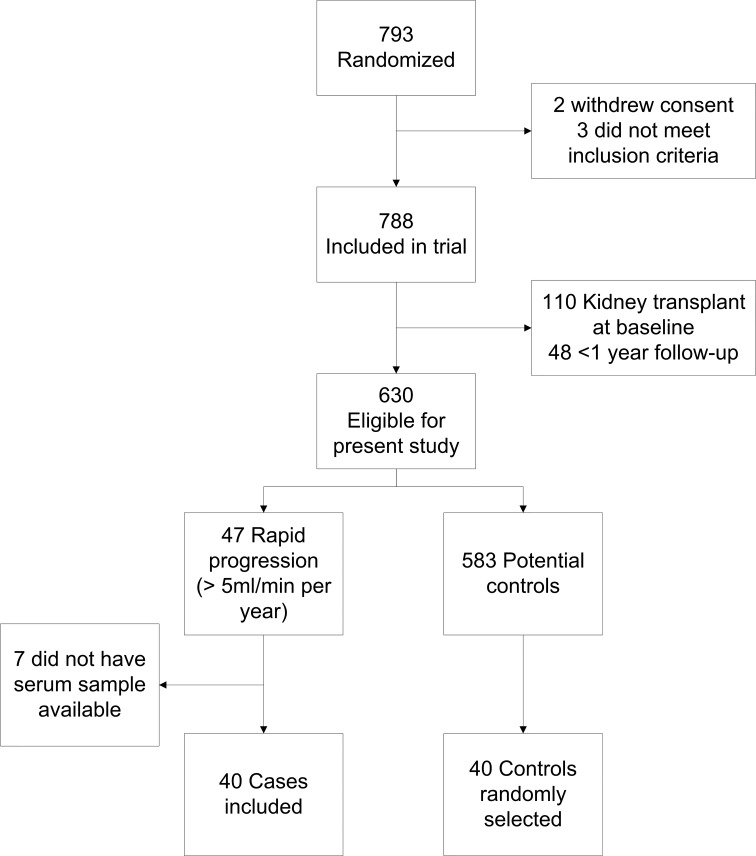
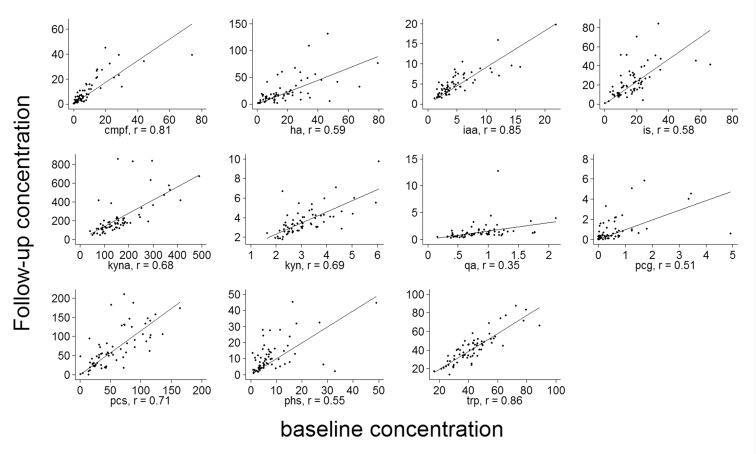
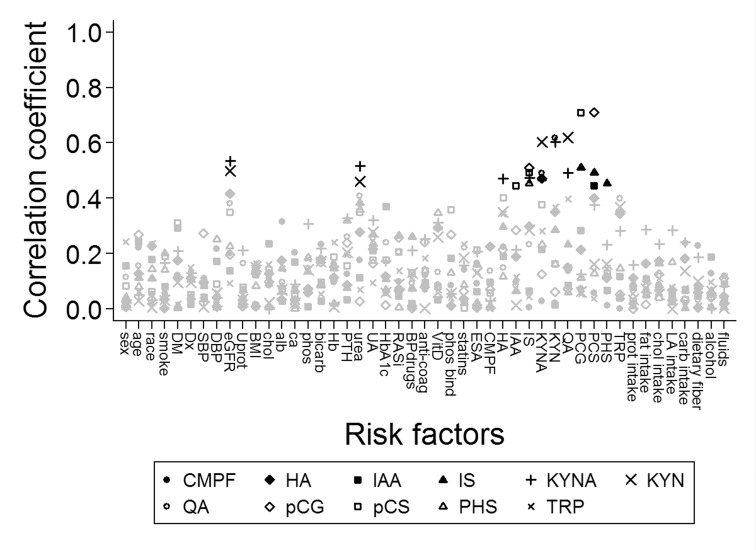
Patients from the MASTERPLAN study, a randomized controlled trial in CKD patients with a creatinine clearance between 20 and 70 ml/min per 1.73m2, were selected based on their rate of eGFR decline during the first five years of follow-up. They were categorized as rapid (decline >5 ml/min per year) or slow progressors. Concentrations of eleven uremic solutes were obtained at baseline and after one year of follow-up. Logistic regression was used to compare the odds for rapid to slow progression by uremic solute concentrations at baseline. Variability in uremic solute levels was assessed using scatter plots, and limits of variability were calculated.
In total, 40 rapidly and 40 slowly progressing patients were included. Uremic solutes were elevated in all patients compared to reference values for healthy persons. The serum levels of uremic solutes were not associated with rapid progression. Moreover, we observed substantial variability in solute levels over time.
Elevated concentrations of uremic solutes measured in this study did not explain differences in rate of eGFR decline in CKD patients, possibly due to lack of power as a result of the small sample size, substantial between patient variability, and variability in solute concentrations over time. The etiology of intra-individual variation in uremic solute levels remains to be elucidated.
迄今为止,已列出超过150种可能的尿毒症溶质,但其在慢性肾脏病(CKD)进展中的作用大多未知。在此,研究了一组选定的尿毒症溶质与CKD患者病情进展之间的关联。
从MASTERPLAN研究中选取患者,该研究是一项针对肌酐清除率为每1.73平方米20至70毫升/分钟的CKD患者的随机对照试验,根据他们在随访的前五年中估算肾小球滤过率(eGFR)的下降速度进行选择。他们被分类为快速进展者(每年下降>5毫升/分钟)或缓慢进展者。在基线和随访一年后获取11种尿毒症溶质的浓度。使用逻辑回归比较基线时尿毒症溶质浓度下快速进展与缓慢进展的几率。使用散点图评估尿毒症溶质水平的变异性,并计算变异限度。
总共纳入了40名快速进展患者和40名缓慢进展患者。与健康人的参考值相比,所有患者的尿毒症溶质均升高。尿毒症溶质的血清水平与快速进展无关。此外,我们观察到溶质水平随时间有很大变异性。
本研究中测得的尿毒症溶质浓度升高并不能解释CKD患者eGFR下降速度的差异,这可能是由于样本量小、患者之间存在较大变异性以及溶质浓度随时间变化而导致的检验效能不足。尿毒症溶质水平个体内变异的病因仍有待阐明。