Hachiya Tsuyoshi, Kamatani Yoichiro, Takahashi Atsushi, Hata Jun, Furukawa Ryohei, Shiwa Yuh, Yamaji Taiki, Hara Megumi, Tanno Kozo, Ohmomo Hideki, Ono Kanako, Takashima Naoyuki, Matsuda Koichi, Wakai Kenji, Sawada Norie, Iwasaki Motoki, Yamagishi Kazumasa, Ago Tetsuro, Ninomiya Toshiharu, Fukushima Akimune, Hozawa Atsushi, Minegishi Naoko, Satoh Mamoru, Endo Ryujin, Sasaki Makoto, Sakata Kiyomi, Kobayashi Seiichiro, Ogasawara Kuniaki, Nakamura Motoyuki, Hitomi Jiro, Kita Yoshikuni, Tanaka Keitaro, Iso Hiroyasu, Kitazono Takanari, Kubo Michiaki, Tanaka Hideo, Tsugane Shoichiro, Kiyohara Yutaka, Yamamoto Masayuki, Sobue Kenji, Shimizu Atsushi
From the Division of Biomedical Information Analysis (T.H., R.F., Y.S., H.O., K. Ono, M. Satoh, A.S.), Division of Biobank and Data Management (T.H., Y.S., M. Satoh), Division of Clinical Research and Epidemiology (K. Tanno, K. Sakata), Division of Innovation and Education (A.F.), Division of Community Medical Supports and Health Record Informatics (M. Satoh), and Division of Public Relations and Planning (R.E.), Iwate Tohoku Medical Megabank Organization (M. Sasaki, S.K., K. Ogasawara, M.N., J. Hitomi, K. Sobue), Iwate Medical University, Japan; Laboratory for Statistical Analysis (Y. Kamatani, A.T.), RIKEN Center for Integrative Medical Sciences, Kanagawa, Japan (M.K.); Laboratory for Omics Informatics, Omics Research Center, National Cerebral and Cardiovascular Center, Osaka, Japan (A.T.); Department of Environmental Medicine (J. Hata), Department of Medicine and Clinical Science (J. Hata, T.A., T.K.), and Center for Cohort Studies (J. Hata, T.N., T.K.), Graduate School of Medical Sciences, Kyushu University, Fukuoka, Japan; Epidemiology and Prevention Group, Center for Public Health Sciences, National Cancer Center, Tokyo, Japan (T.Y., N.S., M.I., S.T.); Department of Preventive Medicine, Faculty of Medicine, Saga University, Japan (M.H., K. Tanaka); Department of Public Health, Shiga University of Medical Science, Japan (N.T., Y. Kita); Laboratory of Molecular Medicine, Human Genome Center, Institute of Medical Science, The University of Tokyo, Japan (K.M.); Department of Preventive Medicine (K.W.) and Department of Epidemiology (H.T.), Nagoya University Graduate School of Medicine, Japan; Department of Public Health Medicine, Faculty of Medicine, University of Tsukuba, Ibaraki, Japan (K.Y.); Department of Preventive Medicine and Epidemiology (A.H.), Department of Biobank (N.M.), and Department of Integrative Genomics (M.Y.), Tohoku Medical Megabank Organization, Tohoku University, Sendai, Japan; Faculty of Nursing Science, Tsuruga Nursing University, Fukui, Japan (Y. Kita); Public Health, Department of Social Medicine, Osaka University Graduate School of Medicine, Japan (H.I.); Division of Epidemiology and Prevention, Aichi Cancer Center Research Institute, Nagoya, Japan (H.T.); and Hisayama Research Institute for Lifestyle Diseases, Fukuoka, Japan (Y. Kiyohara).
Stroke. 2017 Feb;48(2):253-258. doi: 10.1161/STROKEAHA.116.014506. Epub 2016 Dec 29.
The prediction of genetic predispositions to ischemic stroke (IS) may allow the identification of individuals at elevated risk and thereby prevent IS in clinical practice. Previously developed weighted multilocus genetic risk scores showed limited predictive ability for IS. Here, we investigated the predictive ability of a newer method, polygenic risk score (polyGRS), based on the idea that a few strong signals, as well as several weaker signals, can be collectively informative to determine IS risk.
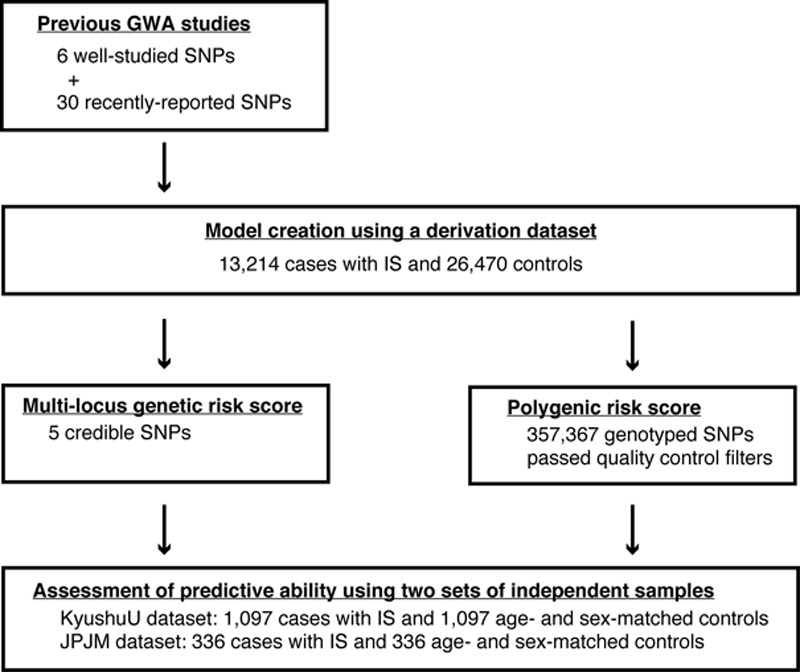
We genotyped 13 214 Japanese individuals with IS and 26 470 controls (derivation samples) and generated both multilocus genetic risk scores and polyGRS, using the same derivation data set. The predictive abilities of each scoring system were then assessed using 2 independent sets of Japanese samples (KyushuU and JPJM data sets).
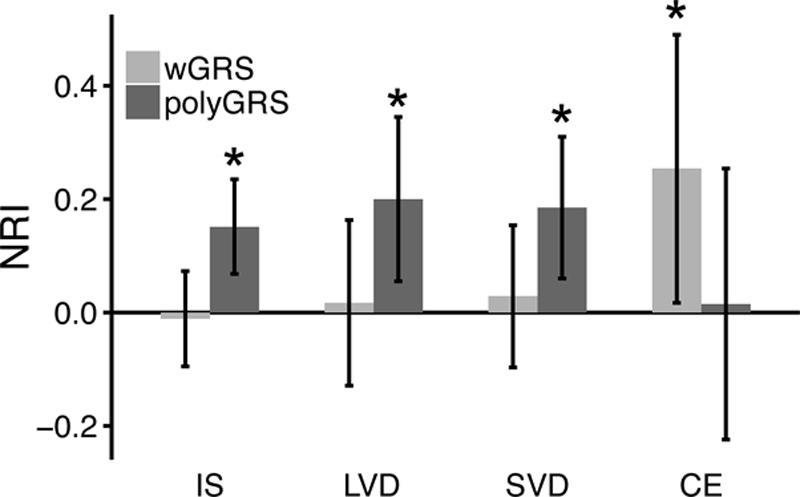
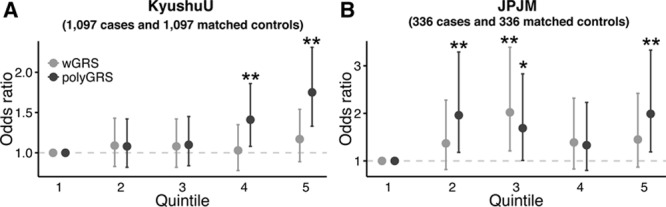
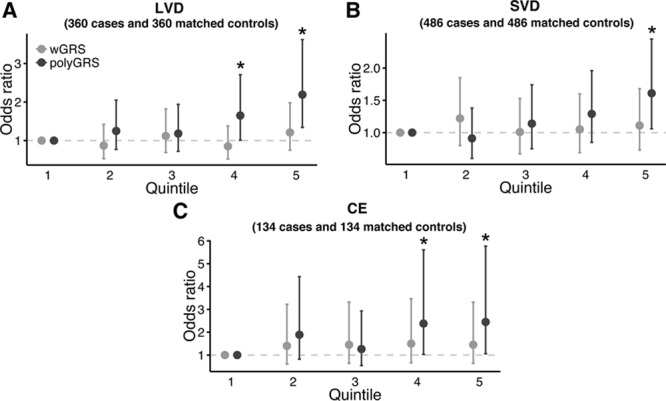
In both validation data sets, polyGRS was shown to be significantly associated with IS, but weighted multilocus genetic risk scores was not. Comparing the highest with the lowest polyGRS quintile, the odds ratios for IS were 1.75 (95% confidence interval, 1.33-2.31) and 1.99 (95% confidence interval, 1.19-3.33) in the KyushuU and JPJM samples, respectively. Using the KyushuU samples, the addition of polyGRS to a nongenetic risk model resulted in a significant improvement of the predictive ability (net reclassification improvement=0.151; P<0.001).
The polyGRS was shown to be superior to weighted multilocus genetic risk scores as an IS prediction model. Thus, together with the nongenetic risk factors, polyGRS will provide valuable information for individual risk assessment and management of modifiable risk factors.
预测缺血性卒中(IS)的遗传易感性有助于识别高危个体,从而在临床实践中预防IS。此前开发的加权多位点遗传风险评分对IS的预测能力有限。在此,我们基于少数强信号以及多个弱信号共同提供信息来确定IS风险这一理念,研究了一种新方法——多基因风险评分(polyGRS)的预测能力。
我们对13214名日本IS患者和26470名对照(推导样本)进行基因分型,并使用相同的推导数据集生成多位点遗传风险评分和polyGRS。然后使用两组独立的日本样本(九州大学样本和JPJM数据集)评估每个评分系统的预测能力。
在两个验证数据集中,polyGRS均与IS显著相关,而加权多位点遗传风险评分则不然。在九州大学样本和JPJM样本中,将polyGRS最高五分位数与最低五分位数进行比较,IS的比值比分别为1.75(95%置信区间为1.33 - 2.31)和1.99(95%置信区间为1.19 - 3.33)。在九州大学样本中,将polyGRS添加到非遗传风险模型中可显著提高预测能力(净重新分类改善 = 0.151;P < 0.001)。
作为IS预测模型,polyGRS优于加权多位点遗传风险评分。因此,与非遗传风险因素一起,polyGRS将为个体风险评估和可改变风险因素的管理提供有价值的信息。