Sood Siddharth, Yu Lijia, Visvanathan Kumar, Angus Peter William, Gow Paul John, Testro Adam Gareth
Siddharth Sood, Department of Gastroenterology and Hepatology, University of Melbourne, Royal Melbourne Hospital, Parkville, VIC 3050, Australia.
World J Hepatol. 2016 Dec 18;8(35):1569-1575. doi: 10.4254/wjh.v8.i35.1569.
To investigate whether a novel immune function biomarker QuantiFERON-Monitor (QFM) can identify cirrhotic patients at greatest risk of infection.
Adult cirrhotic patients on the liver transplant waiting list were recruited for this observational cohort study from a tertiary liver transplant referral unit. The immune function biomarker, QFM was performed using the same method as the widely available Quantiferon-gold assay, and measures output in interferon gamma in IU/mL after dual stimulation of the innate and adaptive immune systems. Ninety-one cirrhotic patients were recruited, with 47 (52%) transplanted on the day of their QFM. The remaining 44 (48%) were monitored for infections until transplant, death, or census date of 1 February 2014.
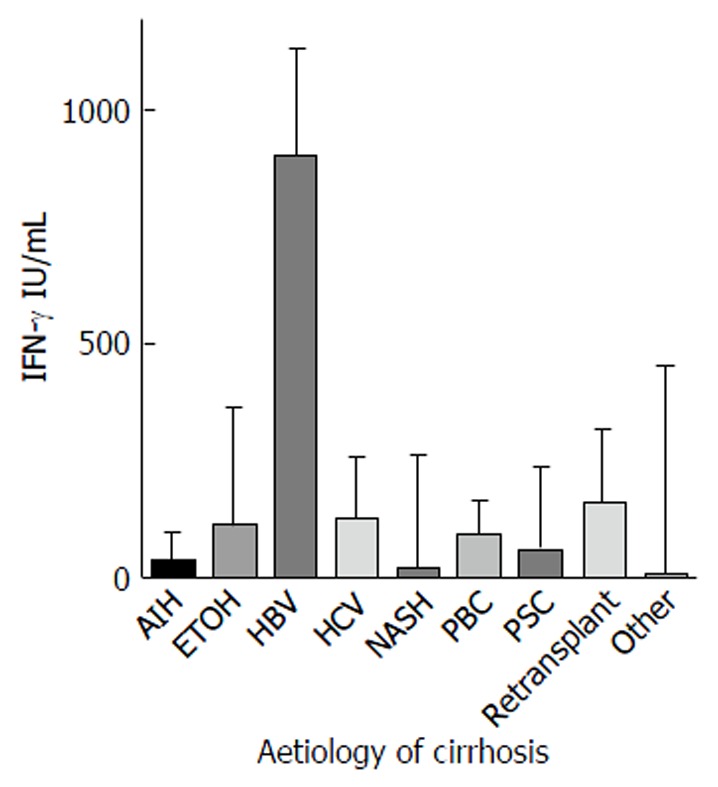
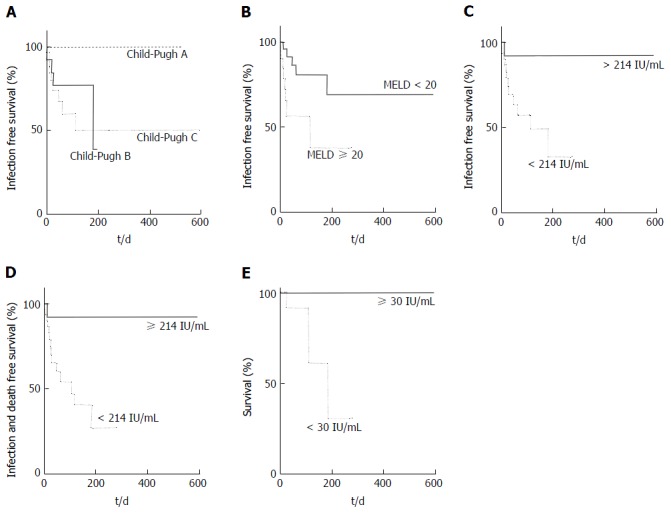
Cirrhotic patients express a median QFM significantly lower than healthy controls (94.5 IU/mL 423 IU/mL), demonstrating that they are severely immunosuppressed. Several factors including model for end stage liver disease, presence of hepatocellular carcinoma, bilirubin, international normalized ratio and haemoglobin were associated with QFM on univariate analysis. Disease aetiology did not appear to impact QFM. On multivariate analysis, only Child-Pugh score and urea were significantly associated with a patient's immune function as objectively measured by QFM. In the 44 patients who were not transplanted immediately after their blood test and could be monitored for subsequent infection risk, 13 (29.5%) experienced a pre-transplant infection a median 20 d (range 2-182) post-test. QFM < 214 IU/mL was associated with HR = 4.1 ( = 0.01) for infection. A very low QFM < 30 IU/mL was significantly associated ( = 0.003) with death in three patients who died while awaiting transplantation (HR = 56.6).
QFM is lower in cirrhotics, allowing objective determinations of an individual's unique level of immune dysfunction. Low QFM was associated with increased susceptibility to infection.
研究一种新型免疫功能生物标志物定量干扰素监测仪(QFM)能否识别出感染风险最高的肝硬化患者。
从一家三级肝移植转诊单位招募了肝移植等待名单上的成年肝硬化患者,进行这项观察性队列研究。免疫功能生物标志物QFM采用与广泛使用的金标定量干扰素检测相同的方法进行检测,测量先天和适应性免疫系统双重刺激后干扰素γ的输出量,单位为IU/mL。招募了91例肝硬化患者,其中47例(52%)在进行QFM检测当天接受了移植。其余44例(48%)在移植、死亡或2014年2月1日普查日期之前接受感染监测。
肝硬化患者的QFM中位数显著低于健康对照者(94.5 IU/mL对423 IU/mL),表明他们存在严重的免疫抑制。单因素分析显示,包括终末期肝病模型、肝细胞癌的存在、胆红素、国际标准化比值和血红蛋白在内的几个因素与QFM相关。疾病病因似乎不影响QFM。多因素分析显示,只有Child-Pugh评分和尿素与通过QFM客观测量的患者免疫功能显著相关。在血液检测后未立即移植且可监测后续感染风险的44例患者中,13例(29.5%)在检测后中位数20天(范围2 - 182天)发生了移植前感染。QFM < 214 IU/mL与感染的风险比(HR)为4.1(P = 0.01)相关。在等待移植期间死亡的3例患者中,极低的QFM < 30 IU/mL与死亡显著相关(P = 0.003)(HR = 56.6)。
肝硬化患者的QFM较低,能够客观测定个体独特的免疫功能障碍水平。低QFM与感染易感性增加相关。