Infectious Diseases Unit, Foundation IRCCS Ca' Granda Ospedale Maggiore Policlinico, 20122 Milan, Italy.
Department of Pathophysiology and Transplantation, University of Milano, 20122 Milan, Italy.
Viruses. 2022 Jul 30;14(8):1683. doi: 10.3390/v14081683.
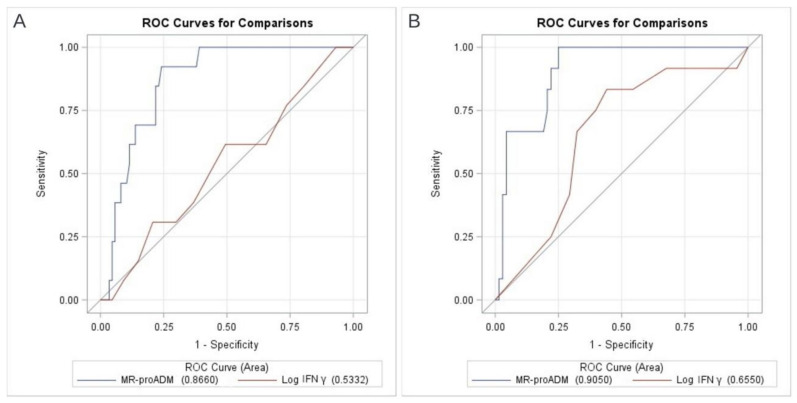
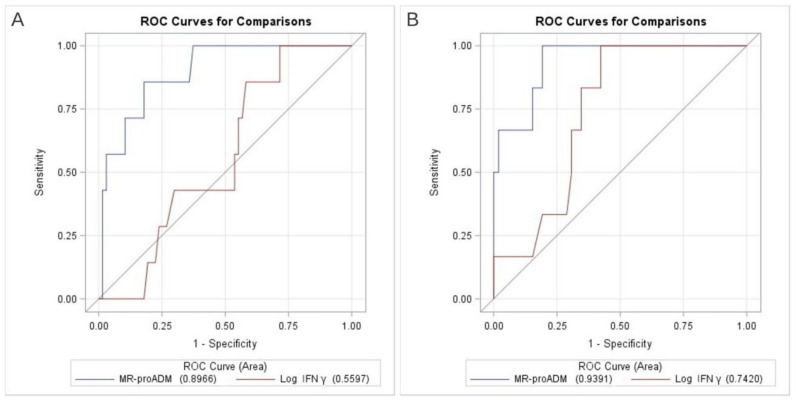
Coagulopathy and immune dysregulation have been identified as important causes of adverse outcomes in coronavirus disease (COVID-19). Mid-region proadrenomedullin (MR-proADM) is associated with endothelial damage and has recently been proposed as a prognostic factor in COVID-19. In non-COVID-19 immunocompromised patients, low in vitro interferon gamma (IFNγ) production correlates with infection risk and mortality. This prospective, monocentric, observational study included adult patients consecutively admitted with radiologic evidence of COVID-19 pneumonia and respiratory failure. MR-proADM and in vitro IFNγ production were measured at T0 (day 1 from admission) and T1 (day 7 from enrollment). One hundred patients were enrolled. Thirty-six percent were females, median age 65 (Q1−Q3 54.5−75) years, and 58% had ≥1 comorbidity. Only 16 patients had received COVID-19 vaccination before hospitalization. At admission, the median PaO2:FiO2 ratio was 241 (157−309) mmHg. In-hospital mortality was 13%. MR-proADM levels differed significantly between deceased and survivors both at T0 (1.41 (1.12−1.77) nmol/L vs. 0.79 (0.63−1.03) nmol/L, p < 0.001) and T1 (1.67 (1.08−1.96) nmol/L vs. 0.66 (0.53−0.95) nmol/L, p < 0.001). In vitro IFNγ production at T0 and T1 did not vary between groups. When only the subset of non-vaccinated patients was considered, both biomarkers at T1 resulted significantly associated with in-hospital mortality. AUROC for MR-proADM at T0 to predict in-hospital mortality was 0.87 (95%CI 0.79−0.94), with the best cut-off point at 1.04 nmol/L (92% sensitivity, 75% specificity and 98% negative predictive value). In patients with COVID-19 pneumonia and different degrees of respiratory failure, MR-proADM at admission and during hospitalization resulted strongly associated with in-hospital mortality. Low in vitro IFNγ production after the first week of hospitalization was associated with mortality in non-vaccinated patients possibly identifying the subgroup characterized by a higher degree of immune suppression.
凝血功能障碍和免疫失调已被确定为冠状病毒病(COVID-19)不良结局的重要原因。中区域原促肾上腺皮质素(MR-proADM)与血管内皮损伤有关,最近被提议作为 COVID-19 的预后因素。在非 COVID-19 免疫功能低下的患者中,体外干扰素 γ(IFNγ)产生减少与感染风险和死亡率相关。这项前瞻性、单中心、观察性研究纳入了连续入院的放射学证据为 COVID-19 肺炎和呼吸衰竭的成年患者。在 T0(入院后第 1 天)和 T1(入组后第 7 天)测量了 MR-proADM 和体外 IFNγ产生。共纳入 100 例患者。36%为女性,中位年龄 65(Q1-Q3 54.5-75)岁,58%有≥1 种合并症。仅有 16 例患者在住院前接受过 COVID-19 疫苗接种。入院时,中位 PaO2:FiO2 比值为 241(157-309)mmHg。住院死亡率为 13%。MR-proADM 水平在 T0(1.41(1.12-1.77)nmol/L 与 0.79(0.63-1.03)nmol/L,p<0.001)和 T1(1.67(1.08-1.96)nmol/L 与 0.66(0.53-0.95)nmol/L,p<0.001)时在死亡组和存活组之间差异有统计学意义。T0 和 T1 时体外 IFNγ产生在组间无差异。仅考虑未接种疫苗的患者亚组时,T1 时的两种生物标志物均与住院死亡率显著相关。T0 时 MR-proADM 预测住院死亡率的 AUROC 为 0.87(95%CI 0.79-0.94),最佳截断值为 1.04 nmol/L(92%敏感性,75%特异性和 98%阴性预测值)。在 COVID-19 肺炎和不同程度呼吸衰竭的患者中,入院时和住院期间的 MR-proADM 与住院死亡率密切相关。在未接种疫苗的患者中,第 1 周后体外 IFNγ产生减少与死亡率相关,可能确定了免疫抑制程度更高的亚组。