Dai Yan, Yang Jingang, Gao Zhan, Xu Haiyan, Sun Yi, Wu Yuan, Gao Xiaojin, Li Wei, Wang Yang, Gao Runlin, Yang Yuejin
Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Science and Peking Union Medical College, 167 Beilishi Road, Beijing, 100037, People's Republic of China.
BMC Cardiovasc Disord. 2017 Jan 4;17(1):2. doi: 10.1186/s12872-016-0442-9.
The incidence, clinical outcomes and antithrombotic treatment spectrum of atrial fibrillation (AF) in patients hospitalized with acute myocardial infarction (AMI) have not been well studied in Chinese population.
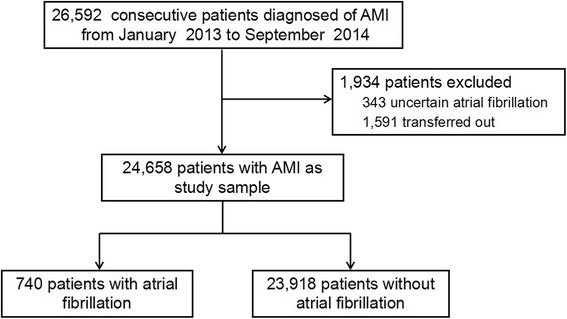
Twenty-six thousand five hundred ninety-two consecutive patients diagnosed with AMI were enrolled in CAMI registry from January 2013 to September 2014. After excluding 343 patients with uncertain AF status and 1,591 patients transferred out during hospitalization, 24,658 patients were finally included in this study and involved in analysis.
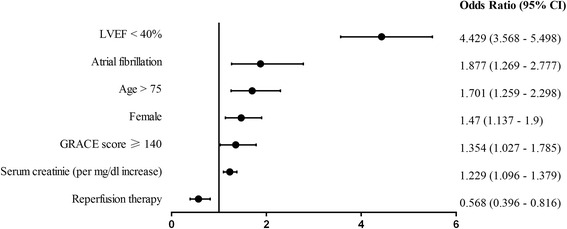
In the CAMI registry, 740 (3.0%) patients were recorded with AF prevalence during hospitalization. Higher-risk baseline clinical profile was observed in patients with AF. These patients were less likely to receive reperfusion/revascularization than those without AF. The in-hospital mortality (including death and treatment withdrawal) was significantly higher in patients with AF than that of without AF (25.2% vs. 7.2%, respectively; p < 0.01). The case of composite of adverse events was similar, which included death, treatment withdrawal, re-infarction, heart failure or stroke (42.1% vs. 16.0%, p <0.01). In multivariate logistic regression analysis, AF was an independent predictor for in-hospital mortality (odds ratio, 1.88; 95% confidence interval: 1.27-2.78) and the composite of adverse events (odds ratio, 2.11; 95% CI: 1.63-2.72). Only 5.1% of patients with AF were treated with warfarin, and 1.7% were treated with both warfarin and dual antiplatelet therapy.
The analysis was based on the CAMI registry in China. The patients hospitalized for AMI who developed AF were at significantly higher risk for in-hospital mortality and other adverse events. However, the anticoagulants including warfarin have been largely underused post hospital discharge.
Clinical Trial Registration: Identifier: NCT01874691 .
急性心肌梗死(AMI)住院患者中房颤(AF)的发病率、临床结局及抗栓治疗情况在中国人群中尚未得到充分研究。
2013年1月至2014年9月,连续纳入26592例诊断为AMI的患者进入中国急性心肌梗死注册研究(CAMI)。排除343例房颤状态不确定的患者及1591例住院期间转出的患者后,最终24658例患者纳入本研究并参与分析。
在CAMI注册研究中,740例(3.0%)患者住院期间记录有房颤患病率。房颤患者基线临床特征风险更高。与无房颤患者相比,这些患者接受再灌注/血管重建治疗的可能性更小。房颤患者院内死亡率(包括死亡和治疗撤药)显著高于无房颤患者(分别为25.2%和7.2%;p<0.01)。不良事件复合情况相似,包括死亡、治疗撤药、再梗死、心力衰竭或卒中(42.1%对16.0%,p<0.01)。多因素逻辑回归分析显示,房颤是院内死亡(比值比,1.88;95%置信区间:1.27 - 2.78)及不良事件复合情况(比值比,2.11;95%CI:1.63 - 2.72)的独立预测因素。仅5.1%的房颤患者接受华法林治疗,1.7%的患者接受华法林和双联抗血小板治疗。
该分析基于中国的CAMI注册研究。因AMI住院且发生房颤的患者院内死亡及其他不良事件风险显著更高。然而,包括华法林在内的抗凝药物出院后使用严重不足。
临床试验注册:标识符:NCT01874691 。