Schidlow David N, Jenkins Kathy J, Gauvreau Kimberlee, Croti Ulisses A, Giang Do Thi Cam, Konda Rama K, Novick William M, Sandoval Nestor F, Castañeda Aldo
Children's National Heart Institute, Children's National Medical Center, George Washington University, Washington, DC.
Department of Cardiology, Boston Children's Hospital, Boston, Massachusetts.
J Am Coll Cardiol. 2017 Jan 3;69(1):43-51. doi: 10.1016/j.jacc.2016.10.051.
Little has been published regarding surgery for transposition of the great arteries (TGA) in the developing world.
This study sought to identify patient characteristics, surgical interventions, institutional characteristics, risk factors for mortality, and outcomes among patients undergoing surgery for TGA in this setting.
Developing world congenital heart surgical programs submitted de-identified data to a novel international collaborative database as part of a quality improvement project. We conducted a retrospective cohort study that included all cases of TGA with intact ventricular septum and TGA with ventricular septal defect performed from 2010 to 2013. Demographic, surgical, and institutional characteristics and their associations with in-hospital mortality were identified.
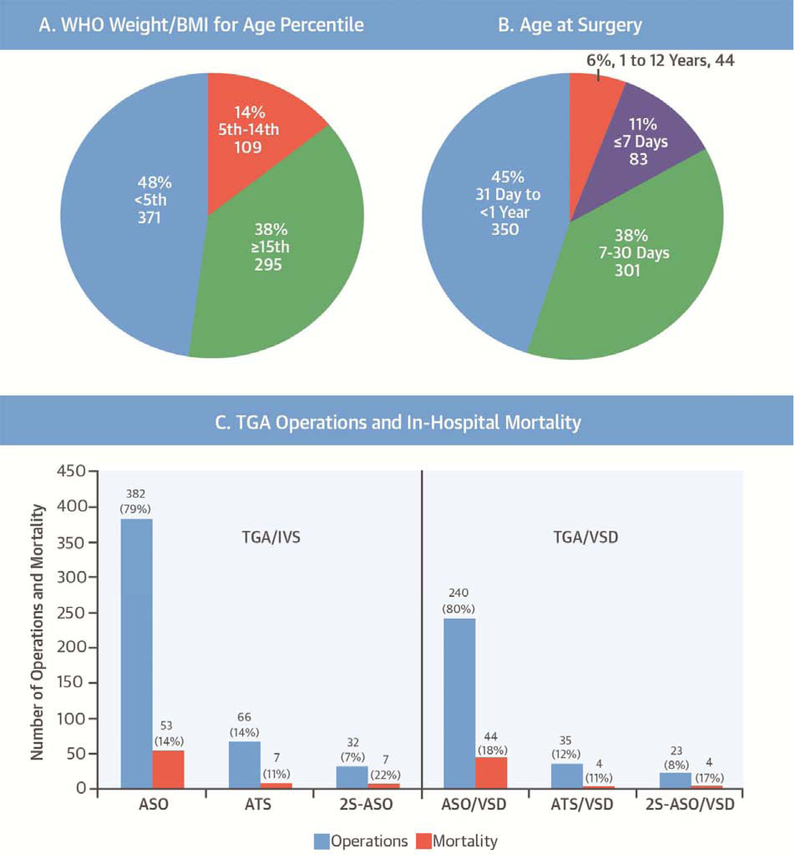
There were 778 TGA operations performed at 26 centers, 480 (62%) for TGA with intact ventricular septum and 298 (38%) for TGA with ventricular septal defect. Most (80%) were single-stage arterial switch operations, but 20% were atrial baffling procedures (atrial switch operation) or 2-stage repairs (pulmonary artery band followed by arterial switch operation). Age at operation was >30 days in one-half of the cases and did not vary significantly with operation type. Survival was 85% and did not significantly vary with age at operation or operation type. Preceding septostomy was infrequently reported (16%) and was not associated with surgical mortality. Mortality was associated with lower World Health Organization weight/body mass index-for-age percentile and lower institutional volume of TGA repair.
Surgical repair of TGA performed in the developing world is associated with an early survival of 85%. Type of surgical repair and age at operation varied considerably, but no associations with mortality were identified. In contrast, poor nutrition and small surgical volume were most strongly associated with mortality. Multicenter collaborative quality improvement efforts may benefit patients with TGA in the developing world.
关于发展中国家大动脉转位(TGA)手术的报道较少。
本研究旨在确定在这种情况下接受TGA手术患者的特征、手术干预措施、机构特征、死亡风险因素及手术结果。
作为一项质量改进项目的一部分,发展中国家的先天性心脏病外科项目将去识别化数据提交至一个全新的国际协作数据库。我们进行了一项回顾性队列研究,纳入了2010年至2013年期间所有室间隔完整的TGA病例以及室间隔缺损的TGA病例。确定了人口统计学、手术及机构特征及其与院内死亡的关联。
26个中心共进行了778例TGA手术,其中480例(62%)为室间隔完整的TGA手术,298例(38%)为室间隔缺损的TGA手术。大多数(80%)为一期动脉调转术,但20%为心房内折流手术(心房调转术)或二期修复术(肺动脉环缩术继以动脉调转术)。一半病例的手术年龄大于30天,且手术类型对此无显著差异。生存率为85%,且与手术年龄或手术类型无显著差异。术前球囊房间隔造口术的报告较少(16%),且与手术死亡率无关。死亡率与较低的世界卫生组织年龄别体重/体重指数百分位数以及较低的机构TGA修复量相关。
在发展中国家进行的TGA手术修复与85%的早期生存率相关。手术修复类型和手术年龄差异很大,但未发现与死亡率有关联。相比之下,营养不良和手术量少与死亡率的关联最为密切。多中心协作质量改进措施可能会使发展中国家的TGA患者受益。