Department of Psychology, The University of Alabama, Box 870348, Gordon Palmer Hall, Tuscaloosa, AL, 35487, USA.
Department of Psychology, REACH Institute, Arizona State University, Tempe, AZ, USA.
J Abnorm Child Psychol. 2017 Oct;45(7):1271-1284. doi: 10.1007/s10802-016-0252-7.
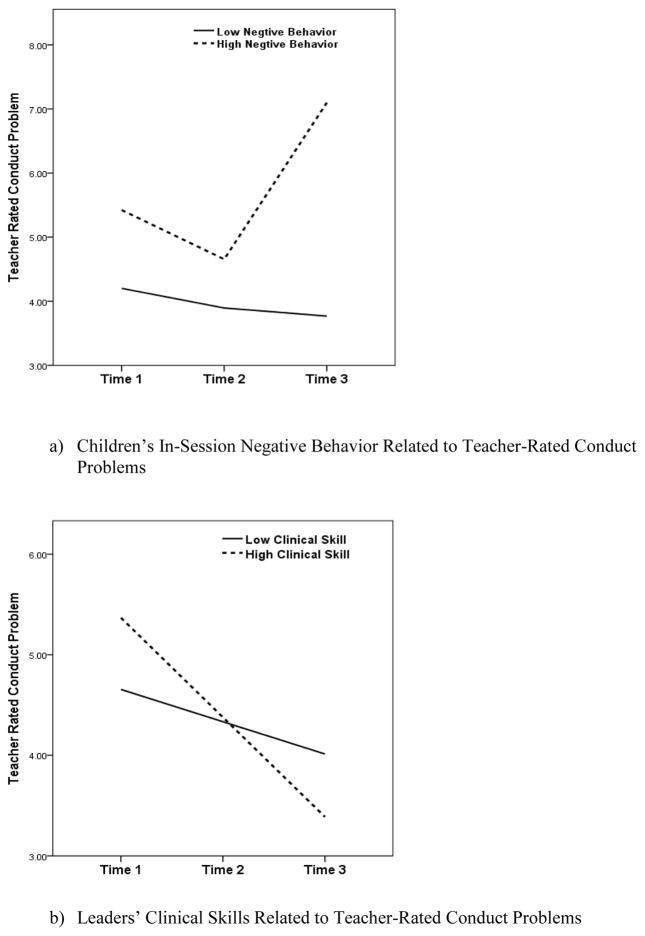
Prior research suggests that under some conditions, interventions that aggregate high-risk youth may be less effective, or at worse, iatrogenic. However, group formats have considerable practical utility for delivery of preventive interventions, and thus it is crucial to understand child and therapist factors that predict which aggressive children can profit from group intervention and which do not. To address these questions we video-recorded group Coping Power intervention sessions (938 sessions), coded both leader and participant behavior, and analyzed both leader and children's behaviors in the sessions that predicted changes in teacher and parent, reports of problem behavior at 1-year follow up. The sample included 180 high-risk children (69% male) who received intervention in 30 separate Coping Power intervention groups (six children assigned per group). The evidence-based Coping Power prevention program consists of 32 sessions delivered during the 4th and 5th grade years; only the child component was used in this study. The behavioral coding system used in the analyses included two clusters of behaviors for children (positive; negative) and two for the primary group leaders (group management; clinical skills). Growth spline models suggest that high levels of children's negative behaviors predicted increases in teacher and parent rated aggressive and conduct problem behaviors during the follow-up period in the three of the four models. Therapist use of clinical skills (e.g., warmth, nonreactive) predicted less increase in children's teacher-rated conduct problems. These findings suggest the importance of clinical training in the effective delivery of evidence-based practices, particularly when working with high-risk youth in groups.
先前的研究表明,在某些情况下,将高风险青少年聚集在一起的干预措施可能效果不佳,甚至更糟,是一种医源性伤害。然而,团体形式对于提供预防干预措施具有相当大的实际效用,因此了解哪些具有攻击性的儿童可以从团体干预中受益,哪些则不能,是至关重要的。为了解决这些问题,我们对团体“应对力量”干预课程(938 节课)进行了视频录制,对领导者和参与者的行为进行了编码,并分析了课程中可以预测教师和家长在 1 年后续跟踪时报告的问题行为变化的领导者和儿童的行为。样本包括 180 名高风险儿童(69%为男性),他们在 30 个不同的“应对力量”干预小组中接受了干预(每个小组分配 6 名儿童)。该循证预防计划“应对力量”由 32 个课程组成,在 4 至 5 年级期间提供;本研究仅使用了儿童部分。分析中使用的行为编码系统包括儿童的两个行为群(积极;消极)和两个主要团体领导者的行为群(团体管理;临床技能)。增长样条模型表明,在四个模型中的三个模型中,儿童的消极行为水平较高,预示着在随访期间教师和家长评定的攻击性行为和行为问题的增加。治疗师使用临床技能(例如,温暖,非反应性)预测了儿童教师评定的行为问题增加较少。这些发现表明,临床培训对于有效实施循证实践至关重要,特别是在团体中为高风险青年提供服务时。