Division of Gastroenterology and Hepatology, Stanford University Medical Center, Stanford, California, USA.
Institute of Clinical Outcomes Research and Education (ICORE), Woodside, California, USA.
Gastrointest Endosc. 2017 Aug;86(2):319-326.e5. doi: 10.1016/j.gie.2016.12.021. Epub 2017 Jan 4.
Bile duct surgery (BDS), percutaneous transhepatic cholangiography (PTC), and ERCP are alternative interventions used to treat biliary disease. Our aim was to describe trends in ERCP, BDS, and PTC on a nationwide level in the United States.
We used the National Inpatient Sample to estimate age-standardized utilization trends of inpatient diagnostic ERCP, therapeutic ERCP, BDS, and PTC between 1998 and 2013. We calculated average case fatality, length of stay, patient demographic profile (age, gender, payer), and hospital characteristics (hospital size and metropolitan status) for these procedures.
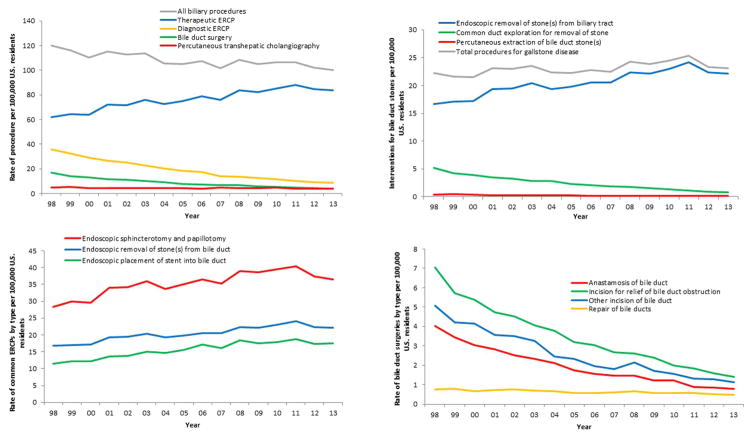
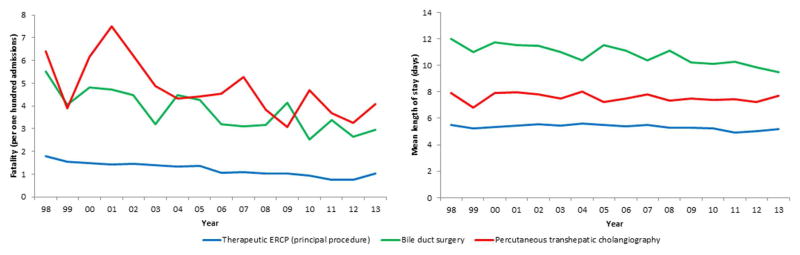
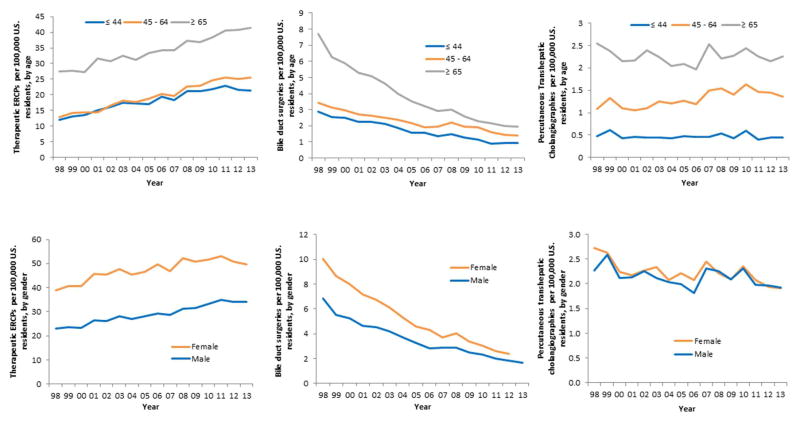
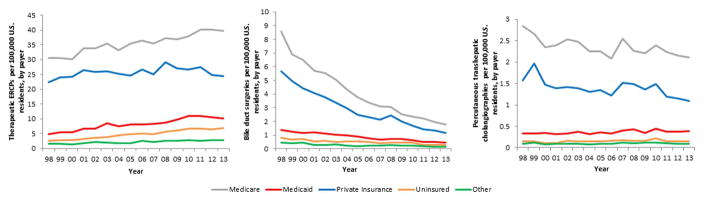
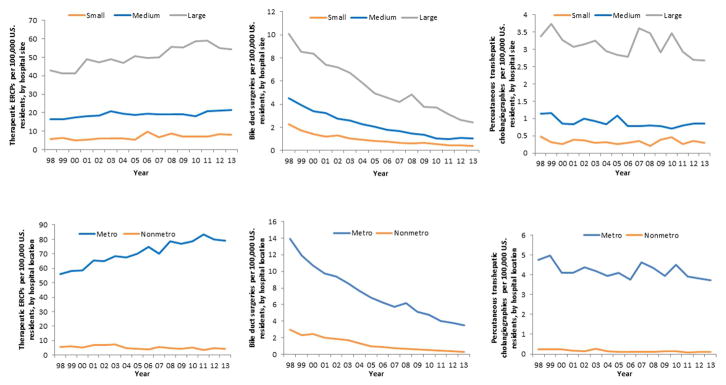
Total biliary interventions decreased over the study period from 119.8 to 100.1 per 100,000. Diagnostic ERCP utilization decreased by 76%, and therapeutic ERCP utilization increased by 35%. BDS rates decreased by 78% and PTC rates by 24%. ERCP has almost completely supplanted surgery for the management of choledocholithiasis. Fatality from ERCP, BDS, and PTC have all decreased, whereas mean length of stay has remained stable. The proportion of Medicare-insured, Medicaid-insured, and uninsured patients undergoing biliary procedures has increased over time. Most of the increase in therapeutic ERCP and decrease in BDS occurred in large, metropolitan hospitals.
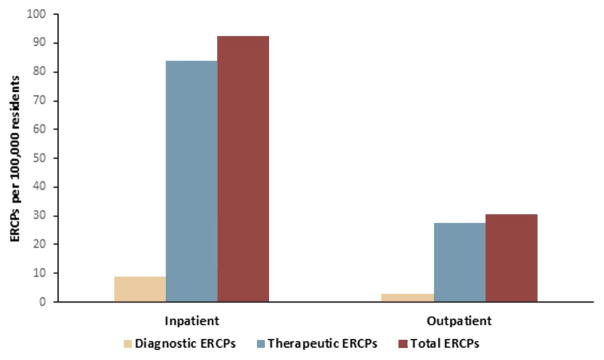
Although therapeutic ERCP utilization has increased over time, the total volume of biliary interventions has decreased. BDS utilization has experienced the most dramatic decrease, possibly a consequence of the increased therapeutic capacity and safety of ERCP. ERCPs are now predominantly therapeutic in nature. Large urban hospitals are leading the shift from surgical to endoscopic therapy of the biliary system.
胆管手术(BDS)、经皮经肝穿刺胆道造影术(PTC)和内镜逆行胰胆管造影术(ERCP)是用于治疗胆道疾病的替代介入方法。我们的目的是描述美国全国范围内 ERCP、BDS 和 PTC 的趋势。
我们使用国家住院患者样本,估计 1998 年至 2013 年期间住院患者诊断性 ERCP、治疗性 ERCP、BDS 和 PTC 的年龄标准化利用趋势。我们计算了这些手术的平均病死率、住院时间、患者人口统计学特征(年龄、性别、付款人)和医院特征(医院规模和大都市地位)。
在研究期间,总胆管介入治疗的数量从每 10 万人 119.8 例减少到 100.1 例。诊断性 ERCP 的使用率下降了 76%,治疗性 ERCP 的使用率增加了 35%。BDS 的使用率下降了 78%,PTC 的使用率下降了 24%。ERCP 几乎完全取代了手术治疗胆总管结石。ERCP、BDS 和 PTC 的病死率均有所下降,而平均住院时间保持稳定。接受胆道手术的医疗保险、医疗补助保险和无保险患者的比例随着时间的推移而增加。治疗性 ERCP 的增加和 BDS 的减少主要发生在大型大都市医院。
尽管治疗性 ERCP 的使用率随着时间的推移而增加,但胆管介入治疗的总数量有所减少。BDS 的使用率下降幅度最大,这可能是 ERCP 治疗能力和安全性提高的结果。ERCP 现在主要是治疗性的。大型城市医院正在引领从胆道手术治疗向内镜治疗的转变。