Frostell Arvid, Hakim Ramil, Thelin Eric Peter, Mattsson Per, Svensson Mikael
Department of Clinical Neuroscience, Karolinska Institutet , Stockholm , Sweden.
Department of Clinical Neuroscience, Karolinska Institutet, Stockholm, Sweden; Department of Neurosurgery, Karolinska University Hospital, Stockholm, Sweden.
Front Neurol. 2016 Dec 23;7:238. doi: 10.3389/fneur.2016.00238. eCollection 2016.
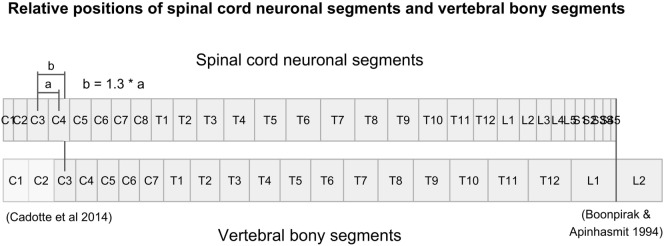
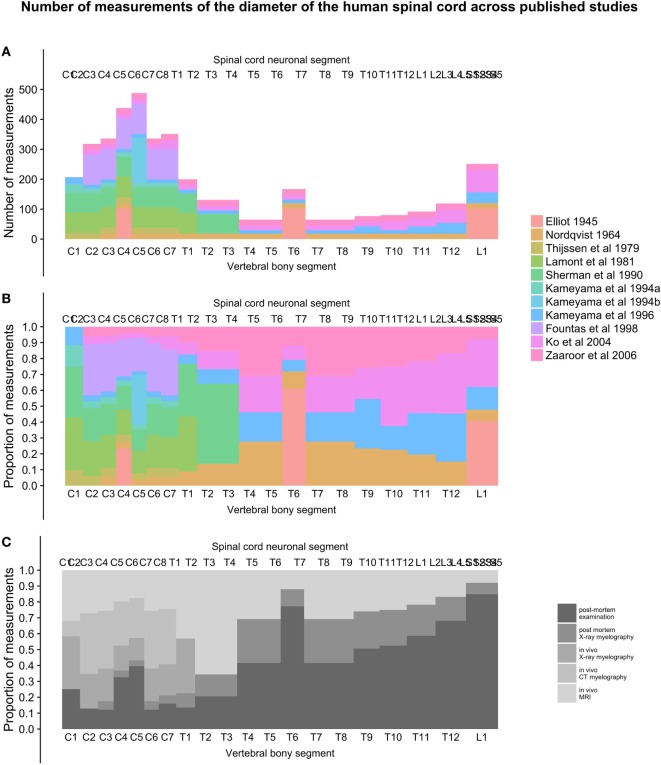
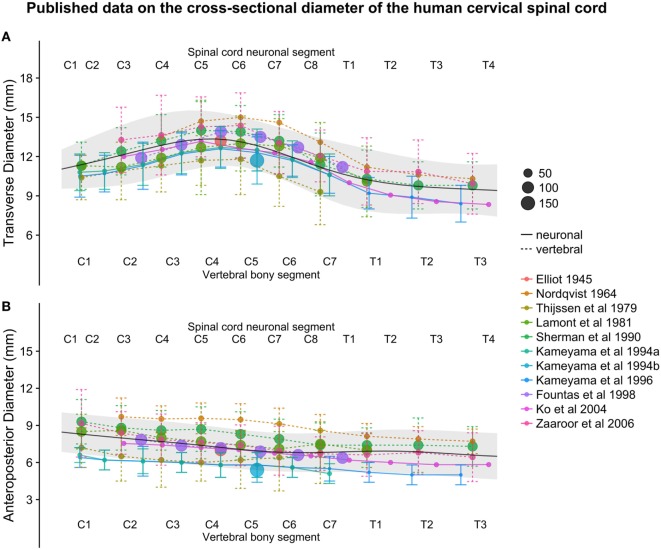
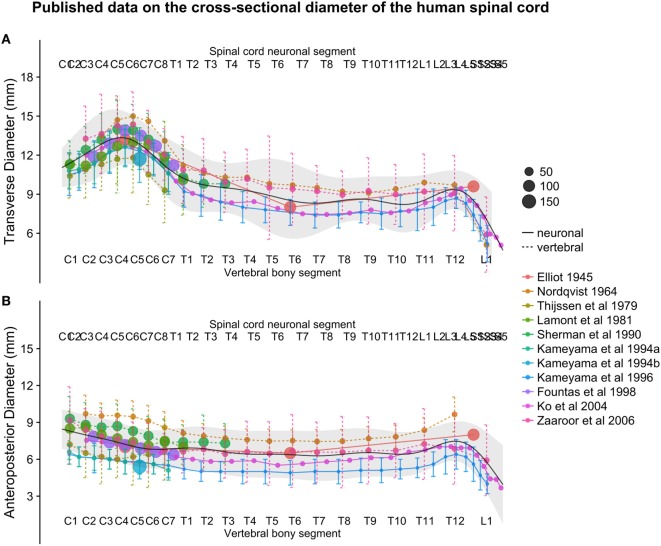
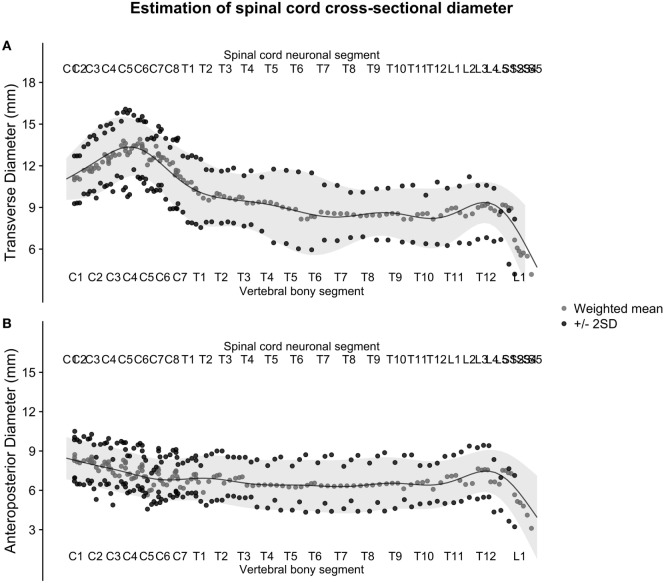
Knowledge of the average size and variability of the human spinal cord can be of importance when treating pathological conditions in the spinal cord. Data on healthy human spinal cord morphometrics have been published for more than a century using different techniques of measurements, but unfortunately, comparison of results from different studies is difficult because of the different anatomical landmarks used as reference points along the craniocaudal axis for the measurements. The aim of this review was to compute population estimates of the transverse and anteroposterior diameter of the human spinal cord by comparing and combining previously published data on a normalized craniocaudal axis. We included 11 studies presenting measurements of spinal cord cross-sectional diameters, with a combined sample size ranging from 15 to 488 subjects, depending on spinal cord level. Based on five published studies presenting data on the lengths of the segments of the spinal cord and vertebral column, we calculated the relative positions of all spinal cord neuronal segments and vertebral bony segments and mapped measurements of spinal cord size to a normalized craniocaudal axis. This mapping resulted in better alignment between studies and allowed the calculation of weighted averages and standard deviations (SDs) along the spinal cord. These weighted averages were smoothed using a generalized additive model to yield continuous population estimates for transverse and anteroposterior diameter and associated SDs. The spinal cord had the largest transverse diameter at spinal cord neuronal segment C5 (13.3 ± 2.2), decreased to segment T8 (8.3 ± 2.1), and increased slightly again to 9.4 ± 1.5 at L3. The anteroposterior diameter showed less variation in size along the spinal cord at C5 (7.4 ± 1.6), T8 (6.3 ± 2.0), and L3 (7.5 ± 1.6). All estimates are presented in millimeters ± 2 SDs. We conclude that segmental transverse and anteroposterior diameters of the healthy human spinal cord from different published sources can be combined on a normalized craniocaudal axis and yield meaningful population estimates. These estimates could be useful in routine management of patients with neurodegenerative diseases as well as for clinical research and experimental applications aimed at surgical spinal cord repair.
在治疗脊髓疾病时,了解人类脊髓的平均大小和变异性可能具有重要意义。关于健康人类脊髓形态计量学的数据已经使用不同的测量技术发表了一个多世纪,但不幸的是,由于在测量中沿头尾轴用作参考点的解剖标志不同,不同研究结果的比较很困难。本综述的目的是通过比较和合并先前发表的关于标准化头尾轴的数据,计算人类脊髓横径和前后径的总体估计值。我们纳入了11项呈现脊髓横截面积测量值的研究,根据脊髓节段水平,合并样本量从15至488名受试者不等。基于5项发表的关于脊髓节段和脊柱长度数据的研究,我们计算了所有脊髓神经节段和椎骨节段的相对位置,并将脊髓大小的测量值映射到标准化的头尾轴上。这种映射使得各研究之间的对齐更好,并允许计算沿脊髓的加权平均值和标准差(SD)。使用广义相加模型对这些加权平均值进行平滑处理,以得出横径和前后径的连续总体估计值以及相关的SD。脊髓在脊髓神经节段C5处横径最大(13.3±2.2),到节段T8时减小至(8.3±2.1),在L3处又略有增加至9.4±1.5。前后径在脊髓C5(7.4±1.6)、T8(6.3±2.0)和L3(7.5±1.6)处沿脊髓的大小变化较小。所有估计值均以毫米±2SD表示。我们得出结论,来自不同已发表来源的健康人类脊髓节段横径和前后径可以在标准化的头尾轴上合并,并得出有意义的总体估计值。这些估计值对于神经退行性疾病患者的常规管理以及旨在脊髓手术修复的临床研究和实验应用可能有用。