Suenari Kazuyoshi, Chao Tze-Fan, Liu Chia-Jen, Kihara Yasuki, Chen Tzeng-Ji, Chen Shih-Ann
Department of Cardiovascular Medicine, Hiroshima University Graduate School of Biomedical Sciences, Hiroshima, Japan. Division of Cardiology, Department of Medicine, Taipei Veterans General Hospital Institute of Clinical Medicine, and Cardiovascular Research Center, National Yang-Ming University Division of Hematology and Oncology, Department of Medicine, Taipei Veterans General Hospital Institute of Public Health and School of Medicine, National Yang-Ming University Department of Family Medicine, Taipei Veterans General Hospital, Taipei, Taiwan.
Medicine (Baltimore). 2017 Jan;96(1):e5597. doi: 10.1097/MD.0000000000005597.
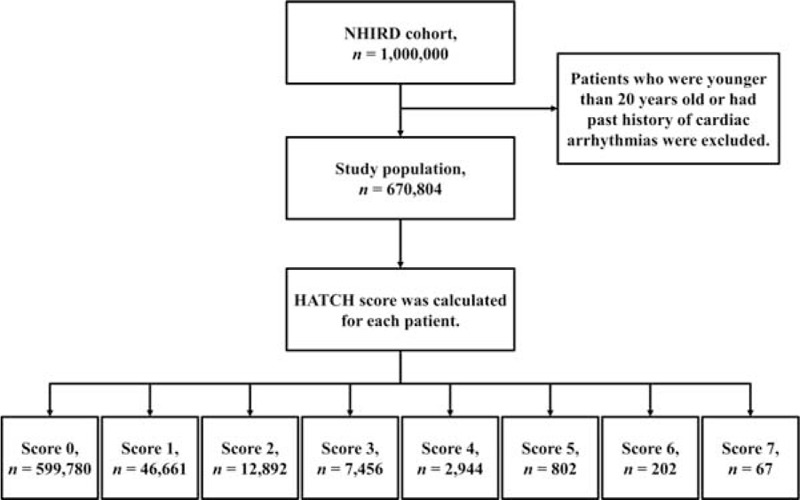
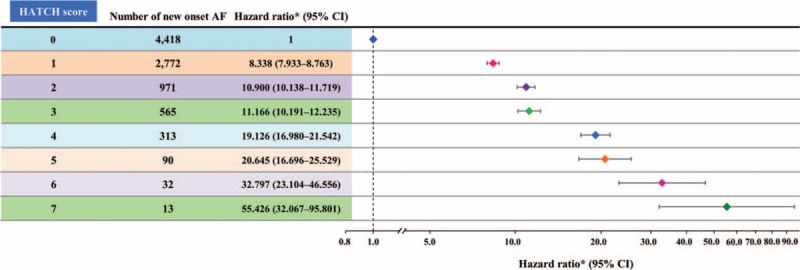
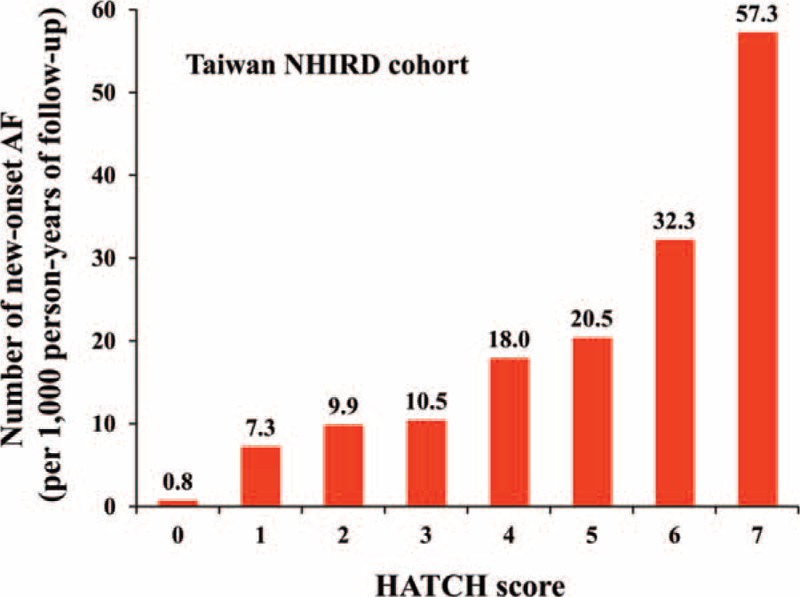
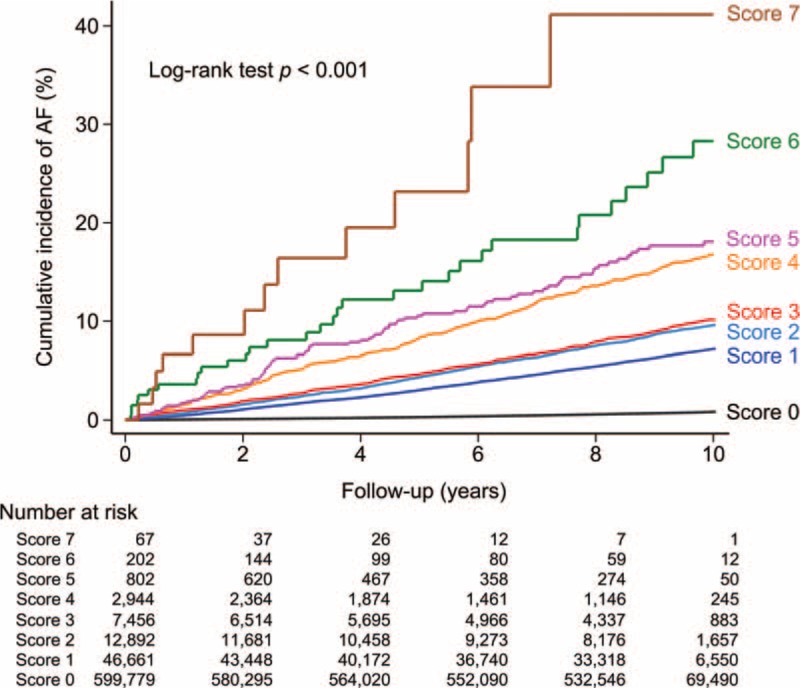
The HATCH score (hypertension <1 point>, age >75 years <1 point>, stroke or transient ischemic attack <2 points>, chronic obstructive pulmonary disease <1 point>, and heart failure <2 points>) was reported to be useful for predicting the progression of atrial fibrillation (AF) from paroxysmal to persistent or permanent AF for patients who participated in the Euro Heart Survey. The goal of the current study was to investigate whether the HATCH score was a useful scheme in predicting new-onset AF. Furthermore, we aimed to use the HATCH scoring system to estimate the individual risk in developing AF for patients with different comorbidities. We used the "Taiwan National Health Insurance Research Database." From January 1, 2000, to December 31, 2001, a total of 670,804 patients older than 20 years old and who had no history of cardiac arrhythmias were enrolled. According to the calculation rule of the HATCH score, 599,780 (score 0), 46,661 (score 1), 12,892 (score 2), 7456 (score 3), 2944 (score 4), 802 (score 5), 202 (score 6), and 67 (score 7) patients were studied and followed for the new onset of AF. During a follow-up of 9.0 ± 2.2 years, there were 9174 (1.4%) patients experiencing new-onset AF. The incidence of AF was 1.5 per 1000 patient-years. The incidence increased from 0.8 per 1000 patient-years for patients with a HATCH score of 0 to 57.3 per 1000 patient-years for those with a HATCH score of 7. After an adjustment for the gender and comorbidities, the hazard ratio (95% confidence interval) of each increment of the HATCH score in predicting AF was 2.059 (2.027-2.093; P < 0.001). The HATCH score was useful in risk estimation and stratification of new-onset AF.
据报道,HATCH评分(高血压<1分>、年龄>75岁<1分>、中风或短暂性脑缺血发作<2分>、慢性阻塞性肺疾病<1分>和心力衰竭<2分>)对于预测参与欧洲心脏调查的患者房颤(AF)从阵发性进展为持续性或永久性房颤很有用。本研究的目的是调查HATCH评分是否是预测新发房颤的有效方案。此外,我们旨在使用HATCH评分系统评估不同合并症患者发生房颤的个体风险。我们使用了“台湾国民健康保险研究数据库”。从2000年1月1日至2001年12月31日,共纳入670804名年龄大于20岁且无心律失常病史的患者。根据HATCH评分的计算规则,对599780名(评分为0)、46661名(评分为1)、12892名(评分为2)、7456名(评分为3)、2944名(评分为4)、802名(评分为5)、202名(评分为6)和67名(评分为7)患者进行了新发房颤的研究和随访。在9.0±2.2年的随访期间,有9174名(1.4%)患者发生新发房颤。房颤的发病率为每1000患者年1.5例。发病率从HATCH评分为0的患者每1000患者年0.8例增加到HATCH评分为7的患者每1000患者年57.3例。在对性别和合并症进行调整后,HATCH评分每增加一分预测房颤的风险比(95%置信区间)为2.059(2.027 - 2.093;P<0.001)。HATCH评分在新发房颤的风险评估和分层中很有用。